 The sleep chronotype is the body’s natural, genetically driven preference for when one falls asleep, wakes up, and reaches peak productivity.
The sleep chronotype is the body’s natural, genetically driven preference for when one falls asleep, wakes up, and reaches peak productivity.
Sleep chronotype refers to an individual’s intrinsic preference for the timing of sleep and wakefulness within the 24-hour day, largely driven by the circadian system.
While a circadian rhythm dictates your 24-hour internal clock, your chronotype is the unique, largely unchangeable way you experience it.
Sleep chronotype refers to an individual’s intrinsic preference for earlier or later timing of sleep and activity within the 24-hour day, reflecting how the circadian system embeds itself into the daily cycle.
Understanding chronotype allows optimization of sleep and productivity to match biology.
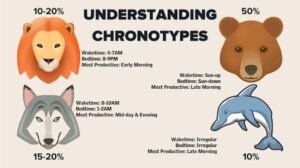
Typically categorized human chronotypes into four animal archetypes: Bear (40% of the population): Sleep and wake preferences align closely with the sun.
They thrive on a traditional 9-to-5 schedule and are most productive between 11:00 AM and 6:00 PM.
Wolf (30% of the population): Classic “night owls” who struggle to wake up early.
They feel energized in the evening and hit their peak productivity in the late afternoon or night.
Lion (15% of the population): Early birds who naturally wake up early (around 5:00 AM) and do their best work before noon, but often feel exhausted by evening.
Dolphin (15% of the population): Light sleepers who often have irregular schedules and struggle with insomnia.
They are usually highly analytical and energetic between 10:00 AM and 2:00 PM.
Working against your chronotype can lead to “circadian misalignment,” which causes chronic fatigue, inflammation, and long-term health risks.
Chronotype is conceptualized as a continuous, normally distributed trait rather than discrete categories, though it is commonly categorized into three groups for clinical and research purposes.
It is commonly categorized into three groups: morning types (“larks”), evening types (“owls”), and intermediate types, with the distribution approximating a normal curve — roughly 20% morning, 20% evening, and 60% intermediate in the general population.
Morning type (“larks”): Tend to go to bed early, wake early, and perform best in the morning hours-Approximately 20% of the general population.
Evening type (“owls”): Tend to go to bed late, wake late, and perform best later in the day. Approximately 20% of the population.
Intermediate (neither) type: Sleep timing falls between the two extremes. Approximately 60% of the population.
Chronotype is strongly influenced by genetics and reflects differences in endogenous circadian period length, with evening types tending to have longer intrinsic circadian periods.
Chronotype is influenced by a combination of genetic, developmental, and environmental factors.
Genetics: Multiple loci have been identified through GWAS, including variants in core clock genes (PER2, CRY, CLOCK, PER3).
Familial advanced sleep phase disorder involves gain-of-function mutations in casein kinase 1 delta and PER2.
Sleep chronotype also depends on the interplay between the circadian oscillator and homeostatic sleep drive, as well as external factors such as light exposure and social schedules.
Physiologically, chronotype correlates with rhythms in body temperature, cortisol secretion, melatonin onset, and cognitive performance timing.
Chronotype shifts systematically across the lifespan.
It becomes progressively later during adolescence, peaking in lateness around age 19, then gradually shifts earlier with advancing age.
Men tend to be later chronotypes than women before age 40, but earlier types after 40.
Assessment Tools
Horne-Östberg Morningness-Eveningness Questionnaire (MEQ): Assesses diurnal preference on a continuous scale; correlates with circadian phase markers.
Munich Chronotype Questionnaire (MCTQ): Focuses on actual sleep timing rather than preference, using mid-sleep on free days (MSF) as the primary chronotype marker.
Importantly, neither self-report measures nor actigraphy directly assess the endogenous circadian clock phase; they are influenced by social schedules and are best considered a starting point before more detailed circadian evaluation.
Clinical Relevance
Evening chronotype is associated with several adverse outcomes:
Reduced sleep quality on polysomnography, including decreased total sleep time, lower sleep efficiency, and less REM sleep compared to morning types.
Social jetlag — the mismatch between social and circadian time on workdays leads to chronic sleep debt, particularly in late chronotypes.
Mental health: Evening chronotype is overrepresented among individuals with depression, bipolar disorder, and ADHD.
Circadian disruption and social jetlag may contribute to impulsivity and inattention.
White matter differences: Diffusion tensor imaging has identified structural brain differences in late chronotypes involving frontal and temporal lobes, cingulate gyrus, and corpus callosum.
Interventions to reduce social jetlag include minimizing evening light exposure, though eveningness itself may represent a lifelong predisposing factor for mood and attentional difficulties.
Age: Chronotype shifts progressively later during adolescence, peaking in “lateness” around age 19, then gradually shifting earlier with advancing age.[5][8]
Sex: Males tend to be later chronotypes than females before age 40, but earlier types after 40.[8]
Light exposure and social/work schedules also modulate expressed chronotype.[2][9]
Assessment Tools
Two widely used instruments exist:
– Morningness-Eveningness Questionnaire (MEQ): Assesses diurnal preference on a scale from definite morning to definite evening type.[1][5]
Munich Chronotype Questionnaire (MCTQ): Calculates mid-sleep on free days (MSF) as a continuous biological measure of circadian phase. These two instruments correlate well (r = −0.73).[1]
Objective validation can be performed using melatonin measurements, with peak melatonin timing differing by up to 4 hours between extreme early and late chronotypes.[6]
Clinical and Health Implications
Evening chronotype is associated with several adverse outcomes:
Reduced sleep quality: Evening types show decreased total sleep time, sleep efficiency, and REM sleep on polysomnography, with increased sleep onset latency and wake after sleep onset.[10]
Social jetlag: Misalignment between an individual’s circadian time and socially imposed schedules (work/school) leads to chronic sleep debt, particularly affecting late chronotypes on weekdays.[2][11]
Psychiatric vulnerability: Evening chronotype is overrepresented among individuals with depression and ADHD. White matter differences in frontal and temporal lobes, cingulate gyrus, and corpus callosum have been observed in late chronotypes.[2][4][12]
Cognitive performance: A “synchrony effect” exists where individuals perform better at their optimal circadian time; evening types appear more cognitively vulnerable at suboptimal times, likely due to social jetlag.[2]
Management Considerations
Reducing evening light exposure can help correct social jetlag, though eveningness itself may represent a lifelong predisposing factor for mood and attentional difficulties.
Aligning work and school schedules with individual chronotype — such as delaying school start times for adolescents — has been advocated to improve circadian alignment and reduce associated health risks.