 The retrograde flow of urine from the bladder toward the kidneys during micturition.
The retrograde flow of urine from the bladder toward the kidneys during micturition.
Normal ureterovesical junction prevents retrograde flow of urine to the kidneys by a flap-valve mechanism.
The flap-valve mechanism relies on the length of the ureter in the bladder wall and sub mucosa, its oblique insertion, and the support of the detrusor muscle behind the ureter.
As intra-vesical pressure rises compression of the ureter results with no back flow of urine in the normal UV junction process.
Primary vesicoureteral reflux results from failure of the development of the UV junction producing an abnormally short tunnel.
The ratio of intramural tunnel length to the ureteral diameter is 5:1.
The above ratio in refluxing ureters is 1.4:1.
In secondary vesicoureteral, which is a much less common process, is associated with increased intra-vesicle Pressure as seen with neurogenic bladder, posterior urethral valves, or dysfunctional voiding.
Ureterovesical junction abnormalities may be congenital as seen with parauretral bladder diverticula or complete ureteral duplication. him not to repair the problem
One of the most common urologic abnormalities in children.
The prevalence is estimated to be about 1%, but may be higher.
Frequency of detection of reflux depends upon the indication for testing that leads to the diagnosis, such that it is diagnosed in about one third of children, mostly females, who are evaluated after UTI, and in about 10% of infants, which are mostly males, with antenatal hydronephrosis.
1-2% of apparently healthy children have this disorder, and it is present in 30-40% of children with urinary tract infection, of whom about 30% have radiological evidence of renal scarring.
Renal scarring in vesiclouteral reflux in childhood may be congenital or acquired, with the former a result of segmental renal dysplasia and mostly seen in boys with high-grade classical funeral reflux and no history of UTI, And the latter a result of renal injury caused by acute pyelonephritis and is seen most frequently in girls.
Patients with reflex nephropathy, termed renal scarring, may be asymptomatic.
Complications of reflux nephropathy include hypertension and proteinuria.
Pregnancy related complications of chronic kidney disease with end-stage renal failure may occur in some patients as a result of reflux nephropathy.
More common in black children than in Caucasians.
Spontaneous resolution of the process occurs commonly, anywhere from 25-80% of patients.
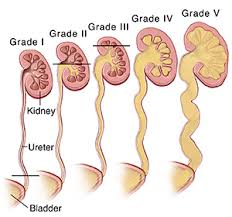
It is graded from I to V: from lowest to most severe.
Grade 1 is the lowest grade with reflux into the urine of only.
Grade 5, associated with marked ureteral tortuosity, calyceal blunting, and severely dilated renal pelvis.
VR in a child with UTI may predispose to pyelonephritis an renal scarring, known as reflux nephropathy.
VR is present in 1/3 of children presenting with febrile UTI and associated with increased risk of renal scarring.
Among children with VR after UTI, antimicrobial prophylaxis reduces risk of recurrence substantially but not of renal scarring (RIVUR Trial Investigators).