 Pancreatic necrosis/necrotizing pancreatitis is a severe complication of acute pancreatitis where severe inflammation cuts off blood flow, causing parts of the pancreas and surrounding tissue to die.
Pancreatic necrosis/necrotizing pancreatitis is a severe complication of acute pancreatitis where severe inflammation cuts off blood flow, causing parts of the pancreas and surrounding tissue to die.
Necrotizing pancreatitis is a severe form of acute pancreatitis characterized by necrosis of the pancreatic parenchyma, peripancreatic tissue, or both, occurring in approximately 10–20% of acute pancreatitis cases and carrying mortality rates of 20–30% when infection develops.
It is a medical emergency that frequently leads to life-threatening infections, sepsis, and multi-organ failure if left untreated.
Severe abdominal pain: Intense, constant pain in the upper abdomen that often radiates to the back and worsens after eating.
Gastrointestinal distress: Nausea, vomiting, and a swollen or highly tender abdomen.
Systemic signs: Fever, chills, and a rapid heart rate, which often signal that the dead tissue has become infected.
Common Causes
Gallstones: Blocking the common bile duct, which backs up digestive enzymes into the pancreas.
Heavy alcohol use: Triggers toxic effects and inflammation within the gland.
Other causes include high triglyceride levels, abdominal trauma, or certain medications.
Diagnosis & Treatment
Diagnosis: Confirmed using blood tests to check enzyme levels and imaging scans (like CT or MRI) to visualize tissue death.
Initial treatment: Requires hospitalization for aggressive intravenous (IV) fluid hydration, pain management, and nutritional support.
Intervention: If the dead tissue becomes infected, medical teams often use a minimally invasive “step-up approach”.
This typically begins with drainage (using a small tube) or an endoscopic procedure to remove dead tissue, and may escalate to surgery (a necrosectomy) only when necessary.
Necrotizing pancreatitis is subdivided anatomically into parenchymal, peripancreatic, and combined subtypes, and temporally into early (<1 week) and late (>1 week) phases.
Associated collections evolve over time:
Acute necrotic collection (ANC): develops within the first 4 weeks; contains solid and fluid components
Walled-off necrosis (WON): develops at or beyond 4 weeks with a well-defined encapsulating wall.
Either may be sterile or infected
Diagnosis
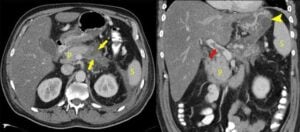
Contrast-enhanced CT (CECT) is the gold standard, with >90% accuracy when >30% glandular necrosis is present.
Necrotic areas demonstrate impaired or absent contrast enhancement.
Contrast-enhanced CT findings may take several days to develop and should generally be obtained when there is persistent systemic response organ failure, or clinical deterioration rather than routinely at admission.
Gas within a necrotic collection on CT is highly suggestive of infection.
Severity is determined by the presence of organ failure.
Mild: no local/systemic complications, no organ failure
Moderately severe: local/systemic complications or transient organ failure (≤48 hours) Severe: persistent organ failure (>48 hours)
Infected necrotizing pancreatitis carries in-hospital mortality exceeding 30%, rising to >40% with concurrent organ failure.
Sterile necrosis has approximately 10% mortality.[
Management
Supportive care remains the cornerstone: fluid resuscitation, nutritional support (enteral nutrition preferred), and monitoring for organ failure.
Prophylactic antibiotics are not recommended.
Multiple randomized controlled trials and meta-analyses have demonstrated no benefit in preventing infected necrosis, reducing systemic complications, or decreasing mortality.
Prophylactic antibiotics are associated with development of multidrug-resistant organisms and fungal superinfection.
Antibiotics for suspected/confirmed infection: When infected necrosis is suspected (fever, leukocytosis, clinical deterioration, gas in collection), broad-spectrum antibiotics with good pancreatic penetration should be initiated — including carbapenems, quinolones, metronidazole, or third-generation or higher cephalosporins.
CT-guided fine-needle aspiration is no longer routinely required but may help guide antibiotic selection in refractory cases.
Indications for Intervention
Infected necrosis is the primary indication for drainage/debridement?
Sterile necrosis rarely requires intervention, except for persistent symptoms (pain, gastric outlet obstruction, biliary obstruction, failure to thrive) at least 4–8 weeks after onset.
In clinically stable patients with infected necrosis, the current consensus favors a 2–4 week course of antibiotics before intervention to allow maturation and encapsulation of the collection, which is associated with decreased mortality.
Step-Up Approach
The minimally invasive step-up approach has replaced open necrosectomy as the standard of care:
Percutaneous catheter drainage or endoscopic transmural drainage (first step) — 23–47% of patients resolve with drainage alone.
Direct endoscopic necrosectomy (DEN) if drainage is insufficient
Surgical debridement (VARD, laparoscopic, or open) if endoscopic approaches fail.
The PANTER trial demonstrated that the step-up approach reduced the combined endpoint of major complications and mortality compared with open necrosectomy (40% vs 69%).
The TENSION trial showed no difference in mortality between endoscopic and surgical step-up approaches, but the endoscopic approach resulted in shorter hospital stays and fewer pancreatico-cutaneous fistulae (5% vs 32%).
The MISER trial similarly favored the endoscopic step-up approach with fewer major complications (12% vs 41%).
The endoscopic step-up approach has become the preferred strategy when anatomically feasible, though percutaneous drainage may be needed for collections extending to the flanks or pelvis.
Early intervention (within 2–4 weeks) carries significantly higher mortality due to the ongoing systemic inflammatory response.
The POSTPONE trial (NEJM 2021) compared immediate versus postponed catheter drainage in infected necrotizing pancreatitis and found that postponement with antibiotics reduced the need for invasive intervention in a substantial proportion of patients.