 Traditionally, 2D mammograms have been performed, which offer a two-dimensional image of the breast.
Traditionally, 2D mammograms have been performed, which offer a two-dimensional image of the breast.
Screening mammograms are usually performed in two standard views, the craniocaudal (CC) and the mediolateral oblique (MLO) views.
Additional diagnostic views including spot compression or variant angles may also be obtained.
The differential attenuation characteristics of tissue allow for the identification of masses, calcifications, and other findings.
Both screen film and, more recently, digital mammography formats have utilized 2D imaging.
Digital Breast Tomosynthesis
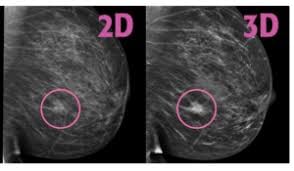
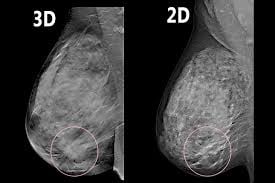
Digital breast tomosynthesis (DBT), colloquially known as 3D mammography, is a newer technology.
DBT acquires multiple mammographic projections serially along an arc and reconstructs this data via post-processing techniques into thin slice images to create a quasi-three-dimensional assessment of the breast.
These reconstructed images result in partial blurring of features outside the selected plane.
The multiple thin images allow radiologists to scroll through each image separately and attenuates the pitfall of superimposed breast tissue in a conventional 2D mammogram.
Multiple studies have shown that the combination of DBT and 2D mammography results in improved performance metrics when compared to 2D mammography alone.
Some mammography units can also produce a synthetic 2D mammogram in post-processing of the DBT data, providing similar information to a conventional 2D mammogram without the additional image acquisition and associated radiation dose.
A meta-analysis involving 42 studies and 2,606,296 patients evaluated breast cancer detection rate (CDR), invasive CDR, recall rate, and positive predictive value (PPV) in combined DBT and 2D mammography, combined DBT and synthetic 2D mammography, DBT alone, and 2D mammography alone.
Combined DBT and 2D mammography and combined DBT and synthetic 2D mammography demonstrated a statistically significant higher CDR (6.36 per 1000 screened, and 7.40 per 1000 screened, respectively), higher invasive CDR (4.53 per 1000 screened, and 5.68 per 1000 screened, respectively), and higher PPV (10.0%, and 16.0%, respectively) compared to 2D mammography alone (CDR 4.68 per 1000 screened, invasive CDR 3.42 per 1000 screened, PPV 7.0%).
Combined DBT and synthetic 2D mammography demonstrated the lowest recall rate (42.3 per 1000 screened compared to 78.8 per 1000 screened for 2D mammography alone.
Because of these improved performance metrics, DBT is increasingly being incorporated into workflows as both a screening and diagnostic tool.
DBT usually requires increased interpretation time compared to a 2D mammogram.
However, given the reduction in recall rates compared to 2D mammography, the utilization of DBT should reduce unnecessary further workup including additional imaging and biopsies and potential associated complications.
Both 2D mammography and DBT use low dose X-rays.
In DBT, the X-ray tube rotates over a set angular range and a low dose radiograph of the breast is performed every few degrees.
While DBT requires acquisition of more X-ray projections, each X-ray projection is achieved at a lower radiation dose than a single 2D mammographic projection.
The resulting average absorbed dose to the glandular breast tissue is the summation of the absorbed doses in all the separate projections.
Etimated radiation dose for DBT versus 2D mammography across multiple vendors, DBT ranged from a slightly lower radiation dose (DBT/2D mammography dose ratio 0.34-1.0) for 1-view DBT to slightly higher radiation dose (dose ratio 0.68-1.17) for 2-view DBT compared to 2D mammography alone
When DBT was combined with 2D mammography and compared to 2D mammography alone, radiation dose ratios ranged from 1.03-1.5 for 1-view DBT plus 2D mammography to 2.0-2.23 for 2-view DBT plus 2D mammography.