 Nephrogenic diabetes insipidus, also known as renal diabetes insipidus, is a form of diabetes insipidus primarily due to pathology of the kidney.
Nephrogenic diabetes insipidus, also known as renal diabetes insipidus, is a form of diabetes insipidus primarily due to pathology of the kidney.
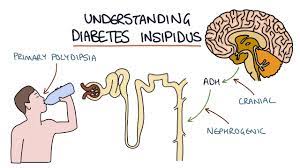
NP is in contrast to central or neurogenic diabetes insipidus, which is caused by insufficient levels of vasopressin (also called antidiuretic hormone, ADH).
Nephrogenic diabetes insipidus is caused by an improper response of the kidney to vasopressin.
This leads to a decrease in the ability of the kidney to concentrate the urine by removing free water.
The clinical manifestation of NDI is similar to neurogenic diabetes insipidus, presenting with polydipsia and polyuria
Dehydration is common manifestation, and incontinence can occur secondary to chronic bladder distension.
Findings include increased plasma osmolarity and decreased urine osmolarity.
Antidiuretic hormone levels are likely to be abnormal or raised.
Nephrogenic diabetes insipidus is most common in its acquired forms.
The most obvious cause is a kidney or systemic disorder, including amyloidosis, polycystic kidney disease, electrolyte imbalance, or some other kidney defect.
The major causes of acquired nephrogenic diabetes insipidus
: in the adult are lithium toxicity and high blood calcium.
About 80% of lithium ingested appears to affect the proximal tubules by entering the collecting tubule cells through sodium channels, accumulating and interfering with the normal response to antidiuretic hormone, in a mechanism that is not yet fully understood.
High blood calcium causes natriuesis and water diuresis, in part by its effect through the calcium-sensing receptor.
Other causes of acquired nephrogenic diabetes insipidus include hypokalemia, post-obstructive polyuria, sickle cell disease or trait, amyloidosis, Sjögren syndrome, renal cystic disease, Bartter syndrome, and various medications, including amphotericin B, orlistat, ifosfamide, ofloxacin, cidofovir, and vaptans.
Hereditary diabetes insipidus can due to defects in genes
resulting of an X-linked genetic defect which causes the vasopressin receptor (also called the V2 receptor) in the kidney to not function correctly.
Less commonly a mutation in the aquaporin 2 gene impedes the normal functionality of the kidney water channel, which results in the kidney being unable to absorb water.
The aquaporin 2 gene mutation is often inherited in an autosomal recessive manner although dominant mutations have been reported.
Differential diagnosis: nephrogenic diabetes insipidus, neurogenic/central diabetes insipidus and psychogenic polydipsia.
These processes may be differentiated by using the water deprivation test.
Assays for antidiuretic hormone can aid in diagnosis.
If the patient is able to concentrate urine following administration of desmopressin, then the cause of the diabetes insipidus is neurogenic diabetes insipidus; if no response occurs to desmopressin, then the cause is likely to be nephrogenic.
Treatment:
Persons with nephrogenic diabetes insipidus will need to consume enough fluids to equal the amount of urine produced.
An underlying cause such as high blood calcium must be corrected to treat nephrogenic diabetes insipidus.
The first line of treatment is hydrochlorothiazide and amiloride.
Patients may also consider a low-salt and low-protein diet.
Thiazide diuretics are used in treatment because diabetes insipidus causes the excretion of more sodium than water, while maintaining the corticomedullary gradient, which is not maintained when using loop diuretics.
The maintained corticomedullary gradient allows more absorption of water in the collecting duct, improving the blood osmolarity and prevents hypernatremia.
High serum osmolarity stimulates polydipsia in an attempt to dilute the serum back to normal and provide free water for excreting the excess serum solutes.
Patients experience polyuria, with an excretion of over 2.5 liters of urine per day, and the urine does not have an elevated glucose concentration, as opposed to diabetes mellitus.
One disease features polyuria in which the urine tastes sweet, whereas the other features polyuria in which the urine tastes unremarkable.