Mnnhhhh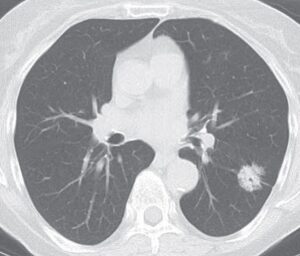 Incidence in the US for individuals age 40-79 years ranges from 4.8-13.7-100,000 person-years for men and 14.4-20.8 her 100,000 person-years for women (Wakelee HA).
Incidence in the US for individuals age 40-79 years ranges from 4.8-13.7-100,000 person-years for men and 14.4-20.8 her 100,000 person-years for women (Wakelee HA).
The incidence of non-small cell lung cancer has more than doubled among nonsmoker to nearly 28% of such cancers (Lim ES).
Responsible for an estimated 100,000 deaths worldwide in 2021.
Lung cancer can be caused by many risk factors other than smoking cigarettes, pipes, or cigars.
These risk factors include exposure to other people’s smoke (called secondhand smoke), radon, air pollution, a family history of lung cancer, and asbestos.
In the United States, about 10% to 20% of lung cancers, or 20,000 to 40,000 lung cancers each year, happen in people who never smoked or smoked fewer than 100 cigarettes in their lifetime.
The median age and diagnosis for patients who are non-smoking individuals is 67 years compared with 70 years in individuals with a history of smoking.
The incidence of lung cancer in non-smoking individuals in the US and worldwide is increasing.
Lung cancer is the third most diagnosed cancer, worldwide, and if lung cancer in non-smoking individuals were classified as a distinct entity, it will be the seventh most common cancer.
Researchers estimate that secondhand smoke contributes to about 7,300 and radon exposure to about 2,900 of these lung cancers.
Radon a colorless gas arises from the radioactive decay of uranium found in rocks and soil and is classified as a class 1 carcinogen.
Up to 21,000 cases of lung cancer related deaths in the US annually are due to radon.
Prior radiotherapy for breast cancer with an observation that suggested 1.474% of patients who receive radiotherapy during breast cancer treatment subsequently developed lung cancer.
Symptoms of lung cancer are the same, whether or not you have smoked.
Some people have general symptoms of not feeling well or feeling tired all the time.
Some people cough frequently, cough up blood, or have chest pain, wheezing, or shortness of breath.
Many patients are asymptomatic and have their tumors discovered incidentally on CT imaging.
People with lung cancer who have never smoked may have a DNA mutation, such as a mutation in the epidermal growth factor receptor (EGFR) gene or other genes.
Targetable genomic variants such as EGFR mutations or ALK1 gene rearrangements, are more common in tumors from non-smoking individuals compared with those with the smoking history (EGFR 43% versus 11%, and ALK1 12% versus 2% in smokers).
Tumor mutation burden, that is the number of somatic mutations in a tumor cell, is lower in lung cancer among non-smoking individuals 0–3 mutations per megabase versus 0 to 30 mutations per megabase.
Cancers caused by these mutations may be treated with targeted therapy.
The median survival among non-smoking individuals with advanced non-small cell lung cancer and actionable genomic alterations can exceed 3 to 5 years, while survival without these genomic alterations is similar to lung cancer in people with a history of smoking (one – two years).
Non-smoking individuals with EGFR mutations or ALK gene rearrangements have improved survival when treated with tyrosine kinase inhibitors compared with chemotherapy.
The U.S. Preventive Services Task Force does not recommend lung cancer screeningfor people who have never smoked.
About 60%-80% of lung cancers found in people who never smoked are adenocarcinomas, about 10% to 20% are squamous cell carcinomas, and 6% to 10% are small cell lung cancers.
Increases the risk of lung cancer in never smokers by 20-30% based on analysis of more than 100 studies.
Environmental tobacco smoke may account for only a small number lung cancer cases in non smokers.
Exposure to rapeseed oil fumes associated with an increased risk of lung cancer in Chinese women with a relative risk of 2.6 (Gao YT).
Exposure to cooking and indoor heating reported to be associated with an increaed risk of lung cancer in Chinese populations (Kleinerman RA).
Risk of developing lung cancer in never smokers associated with a family history of lung with a relative risk of 1.51 (Matakidou A).
Two single nucleotide polymorphisms on chromosome 15q25 associated with an increased risk of developing lung cancer in non smokers(Hung RJ, Amos CL).
Next generation sequencing reveal driver alterations in 95% of never smokers, with the majority having associations with an available targeted therapy.
Targetable genomic variants such as EGFR mutations or ALK gene rearrangements, are more common in tumors from non-smoking individuals compared with those with a smoking history.
Assessment is required for patients with chest symptoms and abnormalities detected on chest x-ray or CT scan of the chest.
Evaluating a primary lesion includes a CT of the chest to assess the primary lesion and for nodal and involvement with metastases.
Biopsy of tumor tissue in lung and or lymph nodes can be performed percutaneously by biopsy or bronchoscopic biopsy often guided by endobronchial ultrasound that confirms the diagnosis.
Molecular testing is performed to aid in decision making about the use of targeted and immunotherapy.
Targeted agents are considered for genetic variants or rearrangements ingenes, including EGFR, ALK, ROS1 and RET.
Characterization by circulating tumor DNA can detect action genomic variants.
Most non-smoking individuals with lung cancer are diagnosed at an advanced stage, typically with unresectable locally advanced disease (stage III) or distant metastasis (stage IV).
Recommended imaging for staging includes CT of the chest, brain imaging, florodeoxyglucose positron emission tomography – CT.