 Caused by an obligate intracellular tick-borne bacteria that infects circulating leukocytes: Anaplasma phagocytophilum.
Caused by an obligate intracellular tick-borne bacteria that infects circulating leukocytes: Anaplasma phagocytophilum.
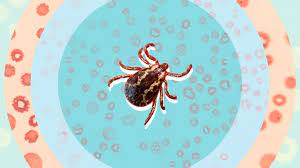
A zoonotic infection transmitted primarily through a bite from the Ixodes scapularis or Ixodes pacificus tick.
Anaplasmosis is due to A. phagocytophilum, transmitted by the Ixodes scapularis, the blacked-leged dear tick.
Occurs in the northeastern U.S. and upper Midwest and is transmitted by Ixodes scapularis tick.
90% of cases occur in eight states: New York, Connecticut, Massachusetts, New Hampshire, Vermont, Maine, Minnesota, and Wisconsin.
Incidence peaks in the summer months when ticks are most active.
In endemic areas annual rate is 16 cases per 100,000 persons.
Patient presents with an acute febrile illness, often with headache.
The illness spectrum ranges from asymptomatic infection to severe disease requiring intensive care.
Incubation period of 5-10 days with presenting symptoms include fever, headache, malaise, headache, nausea, vomiting, cough, and muscle pain.
Typically associated with hepatitis, thrombocytopenia, fever, malaise, myalgias, headache, chills, all symptoms common to viral illnesses.
Laboratory evaluation may reveal leukopenia, thrombocytopenia, and elevated liver function tests.
The diagnosis can be achieved by direct and indirect methods.
Direct diagnostic methods include nucleic acid amplification, testing (NAAT) and microscopy.
The sensitivity of NAAT ranges from 70 to 90% and is highest when the test is performed early in the disease.
The specificity of NAAT approaches 100%.
NAAT is the test of choice.
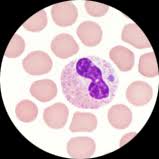
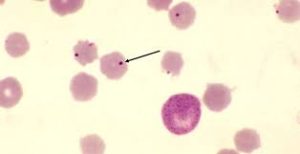
Microscopic examination of a peripheral blood smear can detect interest cytoplasmic inclusions in granulocytes which support the diagnosis.
Sensitivity of microscopic analysis ranges from 25 to 75%.
A. phagocytophilum DNA can be detected in the blood of infected patients by PCR.
Indirect testing, include serological testing as well as evaluation of the peripheral blood count and tests of liver function.
Leukopenia is present in the majority of patients.
Morulae may be identified in neutrophils and peripheral blood smear.
Pulmonary infiltrates may occur.
Rash uncommon.
Doxycycline is the first line treatment, with courses ranging from 7 to 10 days.