 Digital tomosynthesis (DBT) and digital mammography (DM) are both x-ray–based breast imaging modalities, but they differ in image acquisition, reconstruction, and clinical performance.
Digital tomosynthesis (DBT) and digital mammography (DM) are both x-ray–based breast imaging modalities, but they differ in image acquisition, reconstruction, and clinical performance.
Digital breast tomosynthesis (DBT, 3D mammography) generally improves cancer detection and reduces false positives compared with standard digital mammography (DM/ but DM remains adequate and is more widely available and slightly simpler/cheaper in many settings.
DBT is especially useful in dense breasts and higher‑risk women, though large cohort data show its main advantages are lower recall and better detection of earlier‑stage cancers rather than large differences in interval cancer rates for most average‑risk women.
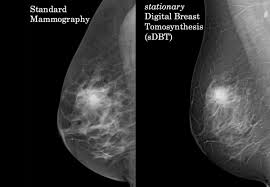
Digital mammography (DM) acquires two‑dimensional projection images (typically cranial caudal and midline oblique) of compressed breast tissue and is the long‑standing standard of care for screening and diagnostic evaluation.
Digital mammography is the standard screening tool and has demonstrated mortality reduction.
Its limitations include reduced sensitivity in women with dense breasts due to tissue overlap, which can obscure lesions or create false positives.
Digital breast tomosynthesis (DBT) acquires multiple low‑dose projections over an arc and reconstructs thin slice images, giving a quasi‑3D view that allows scrolling through the breast and reduces tissue overlap.
Women with heterogeneously or extremely dense breasts benefit from DBT’s ability to unmask lesions obscured by overlapping tissue on DM, improving lesion conspicuity and margin assessment.
For very high‑risk women with extremely dense breasts, DBT has shown significantly lower advanced cancer rates compared with DM, whereas for average‑risk women with less dense breasts, outcome differences are smaller and may not justify universal replacement in all practice environments.
Digital breast tomosynthesis (DBT, or “3D mammography”) acquires multiple low-dose x-ray images from different angles during a single compression.
In smaller diagnostic studies, DBT shows higher sensitivity and specificity than DM, with one series reporting sensitivity 100% vs 73.5% and specificity 94% vs 67.7% for DBT vs DM, respectively.
Large screening cohorts demonstrate that DBT reduces recall rates and modestly increases cancer detection compared with DM over multiple rounds, although interval and advanced cancer rates are similar for most women overall.
DBT is often performed with either a conventional 2D mammogram or a synthetic 2D image reconstructed from the tomosynthesis data, which helps minimize radiation exposure.
Key differences:
Image type: DM is 2D; DBT is quasi-3D (multiple slices).
Sensitivity and specificity: DBT increases cancer detection and reduces recalls, particularly in dense breasts.
Radiation dose: DBT plus DM doubles the dose compared to DM alone, but synthetic 2D images can mitigate this.
DBT requires longer interpretation time but improves diagnostic confidence and reduces unnecessary follow-up.
DBT consistently reduces recall rates and increases cancer detection rates across age groups and breast density categories compared to DM:
DBT offers superior performance over DM in most screening contexts, especially for women with dense breasts, by providing improved lesion visualization and reducing false positives.
DBT tends to lower false‑positive recalls and short‑interval follow‑up recommendations vs DM, which can reduce anxiety and unnecessary imaging/biopsy.
In women with dense breasts or a family history, DBT has been associated with more screen‑detected early‑stage invasive cancers and lower advanced cancer rates in the subgroup with extremely dense breasts and high risk.
DBT usually involves slightly higher radiation dose than a 2D mammogram alone, but protocols using synthetic 2D images keep total dose near or only modestly above standard DM while improving detection.
DM remains more widely available, faster to read, and less expensive in many systems, while DBT requires newer equipment and more interpretation time.
Guideline groups generally view DBT as a preferred or acceptable screening option when available but do not consider DM inadequate when DBT access is limited.
For women with the past history of breast cancer, DBT is a better fiction metrics compared with DM as demonstrated by higher cancer, detection rate, higher invasive, cancer, detection rate, and lower recall rate: however, a lack of significant reduction in interval cancer rates, suggesting they’re both DBY and NDM maybe used for post treatment surveillance.