 Coronary artery aneurysm is an abnormal dilatation of part of the coronary artery.
Coronary artery aneurysm is an abnormal dilatation of part of the coronary artery.
This rare disorder occurs in about 0.3–4.9% of patients who undergo coronary angiography.
Coronary artery aneurysms are defined as a > 50% increase of the vessel diameter.
Some cases are congenital/idiopathic, but most are secondary to atherosclerosis or Kawasaki disease (an immuno-inflammatory disease especially targeting coronary vessels wall).
Potential complications include localized thrombosis, distal embolization, rupture, or late lipid deposits.
Acquired causes include atherosclerosis in adults, Kawasaki disease in children and coronary catheterization.
Drug eluting stents may lead to coronary aneurysms.
The pathophysiology include; disruption of the arterial media, weakening of the arterial wall, increased wall strain and slow dilatation of the coronary artery portion.
Coronary artery aneurysm can also be congenital.
Risk factors:
genetic make-up, especially in patients with congenital coronary artery aneurysms
Coronary artery disease
Vasculitic and connective tissue diseases (Kawasaki and Marfan)
Intracoronary manipulation leading to local wall stress (stent placement, angioplasty, brachytherapy)
Post-infectious as a consequence of direct wall infiltration or immune complex deposition
Diagnosis
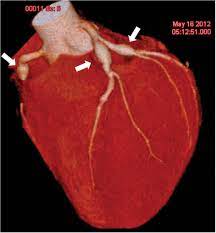
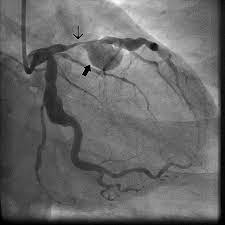
Coronary artery aneurysm is often found coincidentally on coronary angiography.
Other modalities include echocardiography, magnetic resonance imaging and computerized tomography.
Treatment:
Medical management, surgery and percutaneous intervention.
Underlying coronary artery risk factors should be addressed in patients with atherosclerosis.
In patients with risk for embolism or thrombosis, anti-platelet or anticoagulation therapy should be considered.
In patients with Kawasaki disease prompt administration of intravenous immunoglobulin (IVIG) therapy should be given to prevent complication of coronary artery aneurysm.
Prognosis of coronary aneurysm is generally good.
With Kawasaki’s disease that is untreated, there is a 1–2% death rate, from cardiac causes.
The prognosis of coronary artery aneurysm is dependent on its diameter.
The smaller the aneurysm the better the prognosis, with less risk for ischemic myocardial damage and mortality.
Aneurysms with an internal diameter > 8 mm have poorer outcomes, since these aneurysms can be occluded and be associated with complications such as arrhythmias, myocardial infarction, or sudden death.