 A group of disorders characterized by a poorly reversible limitation of airflow that is usually progressive and associated with a persistent inflammatory response in the lungs.
A group of disorders characterized by a poorly reversible limitation of airflow that is usually progressive and associated with a persistent inflammatory response in the lungs.
Affects almost 16,000,000 people in the US and the third leading cause of death.
approximately 392 million people globally have COPD.
Up to 70% of patients with COPD remain undiagnosed.
COPD is the sixth leading cause of disability.
COPD is a clinical syndrome characterized by chronic respiratory symptoms, structural pulmonary abnormalities of the airways, the presence of emphysema, or both, lung function impairment that is poorly reversible, or any combination of the above.
It is characterized by excess mucus production, hypersecretion, and reduced clearance, leading to accumulation in the airways as plugs.
An estimated 20 to 40% of patients with COPD have signs of eosinophilic inflammation, a condition characterized by an increased eosinophil count.
Interleukin-5 is a key type two inflammatory cytokine that drives eosinophil differentiation, growth, maturation, migration, and survival in blood and tissues.
Eosinophilic inflammation alteration, including airway remodeling, mucus plugging, and dysregulation of immune responses are probably important drivers of worsening health and exacerbation in patients with COPD.
Mucous plug that occlude medium to large sized airways in patients with COPD are associated with increased all cause mortality.
Mucous plugs completely include the airways in 25 to 67% of CT scans of individuals with COPD and associated with airflow obstruction, low oxygen saturation, and reduced exercise capacity.
Patients with COPD are at a higher risk than patients without COPD for the development of coexisting conditions that associated with poor outcomes, including death.
Genetic, environmental, and development factors are associated with mechanisms that exert their effects are in childhood and adolescence and can determine low long function in young adults.
Has multiple causes causing airflow limitation that is not fully reversible.
Incompletely reversible airflow obstruction associated with persistent respiratory symptoms including dyspnea, cough, and excessive sputum production.
A common preventable and treatable disease characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities, usually caused by significant exposure to noxious particles or gases.
It is proposed that COPD derives from lifelong changes due to gene-environment relations, smoking, inhalation of pollutants, prematurity, respiratory infections, and dietary insufficiency that modulate development and maintenance of function of the lungs, and include inflammation.
20 to 25% of all COPD patients worldwide have never smoked.
A period of environmental-gene interaction precedes spiral metric airflow limitation.
A third of affected patients worldwide are non-smokers; other environmental pollutants such as smoke from biomass fuel used for cooking and heating are also major environmental risk factors.
A trajectory study demonstrated 50% of COPD among older adults arises from low baseline lung function, rather than from accelerated lung function decline.
Defined as a chronic airflow limitation which is usually both progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases (Pauwels RA).
Definitions include three features:1-a post bronchodilator expiratory volume in 1 second FEV1/forced vital capacity (FVC) ratio of less than 0.70 confirming the presence of airflow limitation, 2-appropriate symptoms including dyspnea, chronic cough, sputum production , or wheezing and 3 significant exposure is to noxious stimuli such is a history of smoking cigarettes or other environmental exposures.
Spirometry is not sensitive to the structural changes associated with COPD, which often occur before lung function decreases below the threshold recommended for defining airflow obstruction: there is increasing consensus that COPD diagnosis should not be based on spirometry alone.
COPD diagnostic scheme should include chest imaging, respiratory symptoms, and spirometry.
Up to half of individuals with a history of cigarette smoking, have evidence of emphysema airway wall thickening on chest CT.
Among individuals without air flow obstruction the risk of developing it on spirometry within five years is two fold higher than those airway wall thickening and four fold greater for those with emphasematous changes on chest CT compared with those who do not have structural abnormalities on chest CT.
COPD is defined by a reduced ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) after bronchodilator use.
Most studies of patients with COPD define a significant exposure to cigarettes at 10 pack years.
More than 75% of COPD diagnoses are related to tobacco smoke, other occupational or environmental particles, or gas exposure such as diesel exhaust and smoke from indoor cooking contribute to the development of COPD.
COPD is a heterogeneous syndrome caused by mechanistically distinct pathophysiological processes including innate and adaptive TH1 type immune response to toxins, microbes, or autoimmunity: persistent THC2 inflammation, anti-protease deficiency, and other mechanisms affecting the airways, alveoli or both resulting in diverse clinical presentations, responses to treatment, and patterns of progression.
COPD‘s severity is associated with the extent to which lung tissue is infiltrated by neutrophils, macrophages, and lymphocytes.
In severe COPD lymphocytes form tertiary lymphoid organs indicating the presence of an adaptive immune response.
Airway remodeling thickens the airway walls involving the epithelium, lamina propria, smooth muscle, and adventitia of the walls of the airways less than 2 mm in diameter.
The number of patent terminal and transitional bronchioles is reduced by 40% in mild to moderate COPD, and by 80% in severe very severe COPD
Defined as an airflow limitation that is not fully reversible.
Dysanapsis is a mismatch of the airway tree caliber to lung size and is believed to arise early in life and is implicated in obstructive lung disease susceptibility, and can be quantified by using CT.
More than 80% of patients affected with airway obstruction have never had a diagnosis of COPD, and even among those with severe obstruction, fewer than half have been diagnosed.
Irreversible or partially reversible airflow limitation, measured by spirometry prior to and after the administration of inhaled bronchodilator is the characteristic physiologic feature of COPD.
Spirometry improves the accuracy of a diagnosis of COPD and results and significant improvement in management.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends using a fixed ratio of 0.7 of the forced expiratory volume in the first second of the force vital capacity (FEV1/FVC) to establish a diagnosis of obstruction.
The degree of air flow limitation is measured using a spirometer: can determine the severity of COPD, assays the response to medications, and follow the progression of the disease.
Patients with COPD the exploratory time maybe too short to allow the respiratory system to return to its relaxation volume.
Airway obstruction can lead to intrinsic PEEP or auto-peep, situation in which the alveolar pressure at the end of expiration is higher than the set PEEP of ventilator.
Associated with an abnormal inflammatory response of the lung to harmful particles or gases.
Is preventable, treatable and usually progressive.
Most patient with COPD die from cardiovascular disease or cancer, but a substantial proportion die from respiratory failure.
Accounted for 5% of all deaths worldwide in 2015, with greater than 90% of COPD deaths occurring in low and middle income countries.
COPD is the third leading cause of mortality globally, causing an estimated 3.23 million deaths in 2019.
Tends to progress, causing a decrease in functional capacity, disability, the need for mechanical ventilation, and eventually death.
Premature birth, severe respiratory infections in childhood, poorly controlled asthma are all associated with lower peak adult lung function, which increases the odds of COPD following exposure by as much is 12.5 fold.
Complex and heterogeneous disease with systemic manifestations and comorbidities that contribute to different pulmonary and extra pulmonary characteristics.
In susceptible persons, exposure to particulate matter, especially tobacco smoke, leads to clinical disease through acceleration of age related decline in pulmonary function, as assessed by the forced expiratory volume in one second (FEV1).
An adaptive immune response to either self antigens or foreign antigens such as bacterial, viral, or fungal, can also contribute on to the pathogenesis of COPD.
Patients with COPD have greater numbers of T lymphocytes and B lymphocytes than healthy persons, as well as B cell infiltration in the walls of terminal bronchioles and areolar tissue
These changes correlate with a reduced number of alveolar attachments to the airway walls, and patients who have COPD with emphysema have a distinct T cell transcriptomic signature.
The above findings indicate autoimmunity in patients with COPD.
The presence of circulating antibodies against elastin and pulmonary epithelium and endothelium and the observation that CD4 positive T cells recognize and respond to elastin by secreting interferon gamma and interleukin-10 in the presence of increased numbers of type 1and type 17 helper T cells secreting cytokines constitute indirect evidence of an acquired immune response in COPD.
A largely preventable and manageable respiratory process that affects more than one in four adults older than 35 years of age.
30 day rehospitalization rate is high and ranges from 20-39%.
Affects 5-22% of adults older than 40 years.
About 14% of US adults have COPD.
Estimated 164,000 deaths in 2016.
Estimated 3.2 million deaths worldwide in 2017.
Prevalence worldwide is around 10%, but varies in different regions.
More than 13 million people have COPD, with another 24 million suspected having undiagnosed disease.
About 3/4 of adults with COPD remain undiagnosed.
WHO estimates that COPD will become the third most common cause of death worldwide by 2030.
Affects 380 million people worldwide.
Lifetime risk of more than 25%.
Annual death rate of 4.8%.
Prevalence is rising driven by an aging population and tobacco smoking, which is the primary risk factor for COPD in high-income countries.
Characterized by chronic airway inflammation resulting in increased mucous production and airway ciliary malfunction.
Third leading cause of death in the U.S.
Third leading cause of death worldwide, and the rate of COPD-related death is increasing.
A leading cause of hospitalization for chronic illness.
Approximately 800,000 hospitalizations annually from COPD.
Rate of death for women with COPD now exceed that of men.
Increasing commonly cause of chronic disability.
In 2005 accounted for approximately one in 20 deaths in the U.S., with smoking estimated to be responsible for 75% of COPD deaths (CDC).
Excess healthcare costs $6,000 annually for every COPD patients in the U.S. (Miller JD).
Accounts for 120,000 deaths annually.
One of the 5 to leading causes of death in the world.
COPD is now the third leading cause of death due to a chronic disease.
COPD affects approximately 29 million Americans.
Accounted for 40.8 deaths per 100,000 person years in 2010 in the US.
6.4% of the US population self reports the diagnosis.
Currently available pharmacotherapy has not altered disease progression, but can reduce the rate of exacerbations or delay such an event.
Third leading cause of death and 12th leading cause of morbidity in the US.
Estimated 24 million persons have COPD in the U.S., based on lung function testing.
Globally fourth leading cause of death.
Approximately 10% of population over the age of 40 years have airflow obstruction of at least moderate degree according to spirometric studies (Buist AS).
Increasing incidence with increasing age.
Not a single entity but all variants have limitation of expiratory airflow.
Diagnosis is based on post bronchodilator spirometry, which detects fixed airway obstruction, or forced expiratory volume in one second to forced vital capacity (FEV1/FVC) ratio of less than 0.7 is the current criteria for diagnosis.
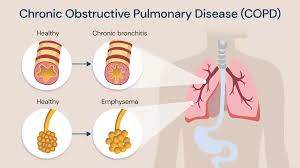
Major disorders include emphysema, chronic bronchitis, bronchiectasis, and asthma.
Persons with COPD are at increased risk of developing dementia.
Administering oxygen therapy to patients with COPD reduced the risk of developing dementia.
Inflammation leads to destruction of respiratory bronchioles, thickening of vascular walls, and parenchymal loss with limitation of airflow, decrements in oxygen and carbon dioxide exchange, elevated pulmonary artery pressures and eventually right ventricular hypertrophy and right heart failure in some patients.
Patients often have dyspnea, chronic cough, and chronic sputum production.
Patients often have a history of exposure to cigarette smoke, heating fuels, or occupational exposure to dust or chemical.
Risks increased with exposure to tobacco smoke and indoor or outdoor pollution.
Additional risk factors include a history of asthma, pulmonary infections, tuberculosis, low socioeconomic group, the tage of greater than 40 years and hereditary gene predisposition.
Approximately 40% of COPD is heritable
Exposure causes continued irritation of the lungs resulting in chronic inflammation of lung parenchyma and a decline in the body’s normal repair processes.
Individual characteristics and the environmental exposure during childhood influences lung function during adolescence and adulthood and may influence the risk of the development of COPD in adulthood.
Comorbidities are common and include lung cancer, ischemic heart disease, anxiety, and depression.
Primary abnormality is an accelerated decline in the forced expiratory volume in one second (FEV1) from the normal rate in adults of approximately 30 ml per year to nearly 60 ml per year.
The key measure of disease progression is expiratory airflow obstruction.
The presence of inflammation in COPD impedes the normal expiratpry process, so that air may build up in the lungs as a result, causing hyperinflation and air trapping.
Air trapping decreases respiratory muscle contractility, increases the release of cytokines and causes dyspnea.
Results in alteration of gas exchange causing carbon dioxide retention and increased secretion of mucus by goblet cells.
The increase in mucus production is a common occurrence but does not occur in all patients with COPD.
Chronic obstructive pulmonary disease (COPD) is a leading cause of death worldwide, and the rate of COPD-related death is increasing.
Treatment goals of stable COPD include reducing symptoms, and reducing risk by preventing disease progression and preventing and treating exacerbations and reducing mortality.
Exacerbations may accelerate disease progression, and approximately half of patients with COPD continue to have exacerbations despite maximal standard care with adequate triple therapy consisting of a glucocorticoid agent, long acting muscarinic antagonist and acting beta agonist.
A subgroup of patients with COPD have evidence of local and systemic type 2 inflammation that is regulated by type 2 helperT cells and innate lymphoid cells and is driven by inflammatory cytokines, including interleukins 4, 5 and 13.
Bronchodilators are separated into 2 major classes by the mechanisms of action and are the mainstay of COPD treatment.
Beta-2 agonists bind to beta-2 adrenergic receptors on airway smooth muscle cells, promoting bronchodilation and increasing ciliary beat frequency.
Muscarinic antagonists block M1 and M3 muscatinic receptors, preventing parasympathetic bronchoconstriction of airway smooth muscle and inhibiting goblet cell mucus secretion.
Although Oral bronchodilators are available, delivery through inhalation improves efficacy and decreases adverse effects.
Long acting muscarinic antagonistsand long-acting beta agonists are preferred over shorter acting bronchodilators, except n patients who have occasional dyspnea only.
Long acting muscarinic antagonists improve symptoms and health status, increase effectiveness of pulmonary rehabilitation, and decrease exacerbations and related hospitalizations.
Long acting muscarinic agents are superior to long acting beta antagonist in decreasing the rate of exacerbations and adverse effects.
Long acting muscarinic agents/long acting beta antagonist combinations have better patient reported outcomes and improve symptoms in health status, as well decreased rates of exacerbations compared with single agent bronchodilator therapy or inhaled corticosteroids plus long acting beta agonist.
Long acting bronchodilator therapy is the cornerstone management for most patients with COPD.
Short-acting bronchodilators include short acting beta2-agonists, albuterol and levalalbuterol and short acting muscarinic antagonist ipratropium.
Short acting bronchodilators maybe used as needed alone or in combination for patients with limited symptoms or activity-specific dyspnea but are not appropriate as scheduled therapies for patients with a history of exacerbation or persistent symptoms.
Escalation to long-acting maintenance broncodilator therapy is recommended for patients using short-acting bronchodilators more than 2-3 times a week.
Triple inhalation therapy of long-acting beta2 agonists plus long acting anti-muscarinic agents plus inhaled corticosteroids remains the cornerstone of treatments for patients with severe COPD.
There is a 1.57 fold increase of bacterial pneumonia in the use of inhaled corticosteroids for COPD.
In some patients with mild disease, and few symptoms, short acting bronchodilators may suffice for symptom control, but in many cases they are used only as rescue medications.
Adding inhaled corticosteroids to long acting beta agonist/long-acting muscarinic agent has not been shown to reduce exacerbations.
No current drug therapy alters the progressive decline in lung function that characterizes COPD.
Exacerbations have prolonged detrimental effects on patients and their clinical course, and preventing such problems are key goals in the management of COPD.
Annual influenza vaccination reduces exacerbations.
Pneumococcal vaccinations support the use of 23-valent pneumococcal polysaccharide vaccine for all patients with COPD or who are current smokers (PPSV-23).
The 13-valent pneumococcal conjugate vaccine is recommended for patients with COPD who is 65 years or olderand for younger patients with frailty will require frequent systemic steroids.
Exacerbation coincide with acute respiratory viral infections including those caused by influenza virus respiratory syncytial virus and picornaviruses.
During exacerbations, even those caused by viral infections the sputum is colonized with bacteria such as streptococcus pneumoniae, H influenza, and Moraxella catarrhalis.
Exacerbations associated with admission to ICU associated with a one year mortality of approximately 50% (Batzlaff CM ETBAL).
A Long-acting β-agonist (LABA) plus a long-acting muscarinic agonist (LAMA) is superior to standard treatment with a LABA plus inhaled corticosteroid (ICS) for the treatment chronic obstructive pulmonary disease (COPD), according to the results of a recent trial.
Combinations of LABA and LAMA for acute exacerbations show improvement in lung function compared with individual components.
Treatment guidelines recommend either a LABA plus an ICS or LAMA for the prevention of COPD exacerbations in high-risk patients, but the efficacy of a LABA-LAMA is unknown.
To compare the methods, the researchers conducted a 52-week randomized, double-blind, double-dummy, noninferiority trial of 3362 patients with a history of at least 1 COPD exacerbation in the previous year. The patients were randomly assigned to either LABA (110 μg) plus LAMA glycopyrronium (50 μg) once daily or to LABA salmeterol (50 μg) plus the the ICS fluticasone (500 μg) twice daily.
Overall, the LABA-LAMA combination was associated with an 11% lower rate of annual COPD exacerbations than the LABA-ICS combination.
LABA-LAMA combination had a longer time to first exacerbation than did the LABA-ICS group-71 days versus 51 days.
Among patients with COPD who had a history of exacerbation during the previous year, indacaterol–glycopyrronium was consistently more effective than salmeterol–fluticasone in preventing exacerbations and was associated with no detectable increase in adverse events.
New bacterial strains are found in about one third of patients in clinics evaluating patients with exacerbations (Sethi S et al).
A correlation exists between bacterial colonization of the lower respiratory airways and elevated levels of inflammatory mediators such as tumor necrosis factor alpha, Interleukin-6 and interleukin-8.
Exacerbations occur 1-2 times per year in the average patient.
Acute exacerbations of COPD require antibiotics for 5 to 10 days, and have a median hospital stay per exacerbation estimated at nine days.
Acute exacerbations of COPD requiring hospitalization are associated with a 30 day rate of death from any cause of 4-30%.
Acute exacerbations accelerate progressive decline in lung function.
COPD exacerbations accelerate loss of lung function, affect quality of life, and are associated with poor survival statistics.
In general COPD exacerbations become more frequent with increasing disease severity, but the single best predictor of such exacerbations is previous exacerbation, suggesting a phenotypical susceptibility to exacerbations, independent of the degree of airflow limitation.
COPD exacerbations are frequently caused by respiratory tract infections and during the acute episodes levels of acute phase proteins and inflammatory cells are elevated.
Many COPD patients, even in the absence of an exacerbation, have evidence of low-grade systemic inflammation with increased levels of inflammatory biomarkers.
With chronic obstructive pulmonary disease concurrent insomnia is an independent risk factor with a fourfold increase in exacerbations, and 11 fold increase in respiratory related emergencies, worse cardiovascular outcomes and a five fold increase in mortality.
Increased levels of inflammatory biomarkers like C-reactive protein, fibrinogen, and leukocytes during stable COPD are associated with poor outcomes.
Overall the FEV1 falls by approximately 33 ml per year in patients with COPD and each acute exacerbation increases the rate of decline by 2 mL per year and by up to seven ml per year in smokers.
Exacerbations indicate instability or worsening of clinical status associated with increased complications, increased likelihood of subsequent exacerbations, worsening of comorbid processes, reduced lung function, reduced quality of life, and increased risk of death.
Patients with a history of a single COPD exacerbation requiring hospitalization have a higher risk of future severe exacerbations.
Risk of mortality can be predicted using the age, dyspnea, airflow obstruction index, which incorporates age, dyspnea scale and FEV1 measures that are easily accessed.
Treatment for exacerbations includes the use of bronchodilators, systemic corticosteroids, antibiotics and oxygen therapy.
Inhaler use is the cornerstone to prevent COPD exacerbations.
Bronchodilators are used clinically to open airways, reduce air trapping, alleviate dyspnea and may improve FEV1.
A combination of long acting beta two agonist with a corticosteroid is better than using either as a single agent to prevent COPD exacerbation recurrences.
TORCH study showed moderate to severe exacerbations of COPD were decreased by 25% in a combination therapy group compared with a single agent group.
Long acting muscarinic agents reduces COPD exacerbations compared to placebo.
Bronchodilators include beta agonists, anti-cholinergics and theophylline.
Beta-2 agonist improve FEV1 and are available as short acting and long acting agents.
Beta agonists increase cyclic AMP and lower intracellular calcium concentrations resulting in relaxation of bronchial and tracheal smooth muscle, which relieves bronchospasm, reduces airway resistance, facilities mucous drainage and increases vital capacity.
The use of systemic corticosteroids in COPD exacerbations evaluated in a Cockrane review demonstrated the change in the forced expiratory volume in the first second and expiration within the first 72 hours was increased in patients given corticosteroids, and there were fewer treatment failures within 30 days, and the duration of hospitalization was significantly shorter as well (Walters JAE et al).
In the above analysis systemic corticosteroids in COPD exacerbation had no effect on mortality, but one extra adverse effect occurs every patients treated, and hyperglycemia was significantly increased.
For inpatients with COPD exacerbations short courses of oral prednisone are appropriate, and inpatients on ventilators intravenous corticosteroids should be utilized.
Exacerbations occur in 5-15% of patients on mechanical ventilation.
Approximately 10% of patients with acute exacerbations of COPD require mechanical ventilation.
In a double-blind, placebo-controlled trial evaluating systemic corticosteroids in patients with COPD exacerbation while on mechanical ventilation, treatment with corticosteroids is associated with a significant reduction in median duration of mechanical ventilation with a shorter median length of ICU stay, and a significant reduction in the rate of noninvasive venilatory failure(Alia I et al).
Patients with moderate to severe COPD who are frequent exacerbators (annual rate of 1. 5 or more exacerbations per year) experience significant greater decline in FEV1 then do infrequent exacerbators (less then 1.5 the exacerbations per year).
Individuals who experience greater than 2.92 exacerbations per year had significantly more hospital admissions and longer lengths of hospital stay than patients who experience less than 2.92 exacerbations per year.
Inhaled glucocorticoids, long-acting beta 2 agonists, and long acting muscarinic antagonists reduce the frequency of acute exacerbations of COPD, but patients receiving all 3 of these medications may still have as many as 1.4 acute exacerbations, on average, each year(Aaron SD et al).
Inhaled corticosteroids (ICSs) does not improve the acceleration rate of lung function decline in patients with mild to severe COPD, but it does reduce frequency of acute exacerbations and improved health status and symptoms of COPD.
Regular treatment with inhaled corticosteroids in patients with and FEV1 of less than 60% improve symptoms and quality-of-life and may reduce exacerbations.
Inhaled corticosteroids may cause alterations in voice quality, candidiasis, and increased risk for pneumonia.
A Long-acting β-agonist (LABA) plus a long-acting muscarinic agonist (LAMA) is superior to standard treatment with a LABA plus inhaled corticosteroid (ICS) for the treatment chronic obstructive pulmonary disease (COPD), according to the results of a recent trial.
Treatment guidelines recommend either a LABA plus an ICS or LAMA for the prevention of COPD exacerbations in high-risk patients, but the efficacy of a LABA-LAMA is unknown.
To compare the methods, the researchers conducted a 52-week randomized, double-blind, double-dummy, noninferiority trial of 3362 patients with a history of at least 1 COPD exacerbation in the previous year. The patients were randomly assigned to either LABA (110 μg) plus LAMA glycopyrronium (50 μg) once daily or to LABA salmeterol (50 μg) plus the the ICS fluticasone (500 μg) twice daily.
Overall, the LABA-LAMA combination was associated with an 11% lower rate of annual COPD exacerbations than the LABA-ICS combination.
LABA-LAMA combination had a longer time to first exacerbation than did the LABA-ICS group-71 days versus 51 days.
Among patients with COPD who had a history of exacerbation during the previous year, indacaterol–glycopyrronium was consistently more effective than salmeterol–fluticasone in preventing exacerbations and was associated with no detectable increase in adverse events.
Estimated that 50-70% of patients with COPD use ICS’s with long-acting beta-adrenergic agonist bronchodilators.
Meta-analyses show a 50-70% increase in risk of pneumonia associated with the use of ICSs in COPD and the risk is mostly associated with high doses of fluticasone proprionare and not budesonide or ciclesonide.
In a randomized trial azithromycin taking daily for one year among selected patients with COPD, when added to usual treatment, decreased the frequency of exacerbations and improve quality of life but caused hearing decrements in a small percentage of patients (Albert RK et al).
Sentinel clinical feature is dyspnea on exertion.
Dyspnea on exertion is usually of insidious onset, but can progress to severe disability over years to decades.
Common symptoms include cough sputum production, chest congestion and wheezing.
Chronic hypoxemia and hypercapnea may cause cor pulmonale and pulmonary hypertension.
Expiratory airflow obstruction can result from narrowing of the airway, associated in asthma, or from loss of elastic recoil of the lung as in emphysema.
The onset of symptoms occurs when the FEV1 falls to approximately half of normal value.
Progression of airway obstruction related to thickening of the airway wall and to the degree to which lumens of airways are filled with exudates and inflammatory response.
Most patients have inspiratory muscle weakness.
Inspiratory muscle weakness probably caused by the presence of mechanical disadvantage of hyperinflation.
Several reports suggest that expiratory muscle strength is impaired decreasing endurance and quality of life in COPD.
Expiratory muscle training can improve muscle strength and increase exercise performance in patients with COPD.
Physical examination may reveal a barrel chest, inspiratory retraction of the lower ribs, known as Hoover’s sign, prolongation of expiration, and use of accessory muscles to breathe.
Secondary to prolonged exposure to toxic gases and particles which are often associated with cigarette smoking.
In developed countries 90% of cases are caused by inhalation of cigarette smoke.
Incidence in lung cancer in smokers with COPD is 4-5 times that reported in smokers without COPD or with chronic bronchitis alone.
Associated with increased risk of systemic illnesses including cardiovascular disease, lung cancer, osteoporosis and depression.
Inhalation of smoke from biomass fuels is an important cause of COPD, especially among women cooking in poorly ventilated homes.
Characterized by inflammation throughout the lung airways, parenchyma and pulmonary vasculature.
Testing for alpha1-antitrypsin should be considered in patients who are young or have a strong family history of COPD.
Only 5% of patients with alpha-1-anti-trypsin deficiency have been diagnosed.
While diagnosis is suspected by history and physical findings, the diagnosis must be confirmed by spirometer studies.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) Classification of severity of airflow limitation in COPD -in patients with FEV/FVC less than 0.70.
GOLD 1:mild FEV1 greater or equal to 80% predicted.
GOLD 2: moderate 50% or less FEV1< 80% predicted
GOLD 3: Severe 30% equal or less FEV1 less than 50% predicted
GOLD 4: very severe FEV1 less than 30% predicted
Spirometry defines airflow obstruction as a ratio of the postbronchodilator FEV1 to FVC of less than 0.70.
FEV1/FVC may decrease with aging with or without diagnosis of COPD.
Spirometry establishes the severity of obstruction according to the FEV1 as a percentage of the predicted normal value.
Oximetry may help identify patients with chronic hypoxemia, those that will benefit from long-term oxygen therapy.
The improvement of lung function with bronchodilators is small relative to measurment eror.
Spirometry is a poor guide for treatment changes and once done needs not be done serially, although an annual examination may provide prognostic information (Niewoehner DE).
A chest x-ray is obtained at initial evaluation to rule out other pulmonary processes.
CT of the chest is not part of an initial evaluation unless one is expecting another diagnosis or surgery for COPD is being considered.
Progression of disease is associated with accumulation of inflammatory cells in airway walls along with inflammatory mucous exudates in airway lumens.
In various parts of the lungs macrophages, neutrophils, CD8+ T cell lymphocytes are increased.
Mediators released by inflammatory cells are leukotrienes, IL-8, TNF and others are capable of damaging the lung.
Two thirds of patients with COPD have serious chronic dyspnea and nearly 25% have total body pain.
Bacterial infection is a factor in 70-75% of exacerbations with up to 60% caused Streptococcus pneumoniae, Haemophilus influenzae or Moraxella catarrhalis.
Atypical organisms such as Chlamydia pneumoniae implicated in about 10% of exacerbations.
Viruses cause about 25-30% of cases of exacerbation.
Acute exacerbations treated with systemic steroids improve FEV1.
Substantial proportion of persons in whom COPD develops have a low FEV1 level in early childhood.
4-6% of adult population has clinically relevant COPD.
Cigarette smoking is the most important risk factor in its development.
Only a small proportion of smokers develop significant clinical COPD.
20% of patients with COPD or die from it are nonsmokers.
Risk factors include burning of biomass fuels for cooking and heating in many developing countries.
Acute exacerbation-characterized by episodic increases in dyspnea, cough and sputum production.
85% of patients have chronic bronchitis and 15% have emphysema.
Guidelines suggest use of inhaled bronchodilators for patients whose COPD is stable but who have respiratory symptoms and FEV1 between 60-80%.
Treatment recommendations includes monotherapy with either long-acting inhaled anticholinergic medications or long-acting beta-agonists for symptomatic patients with severe COPD with FEV1< 60%.
After an acute exacerbation, most patients experience a decrease in quality of life, transitory or permanent, and nearly half of patients discharged from the hospital are readmitted more than once in the following 6 months.
Long acting B agonists (LABAs) and inhaled corticosteroids (ICSs) decrease exacerbations in COPD and possibly decrease mortality.
In randomized controlled trials exacerbation rates but not hospitalizations or mortality were lowered by LABAs-ICSs compared to LABAs alone.
Inhaled short acting B-agonists, such as albuterol, and anticholinergic bronchodilators, such as ipratropium, are equally efficacious in patients with acute exacerbations of COPD. They are also superior to all parenterally administered bronchodilators.
Many patients prefer the short acting Beta2-adrenergic agonist to ipratropium because it is faster acting.
Long-acting Beta2-agonists salmeterol and fomoterol can provide sustained bronchodilation for at least 12 hours.
Inhaled long acting anticholinergic agent tiotropium can provide sustained bronchodilation for at least 24 hours.
Inhaled anticholinergic agents work via local muscarinic receptor blockade, causing relaxation of of airway smooth muscle and decreased airflow obstruction.
Both long actong beta2-agonists and long acting anticholinergic agents when used as monotherapy confer similar benefits.
Long acting anti-cholinergic drugs or long acting beta2 agonists are recommended as first-line maintenance therapy in patients with moderate to severe COPD, as both types of agents reduce symptoms, improve lung function and quality of life and reduce the risk of exacerbations.
The efficacy of wet nebulization and dry aerosol delivery systems are clinically equivalent.
Inhaled steroids are not appropriate in the treatment of acute exacerbation of COPD.
Inhaled corticosteroids therapies utilized to decreases pulmonary inflammation and can be administered as monotherapy or combination treatment with long acting Beta2-agonists.
Inhaled corticosteroid (ICS) recommended, in addition to bronchodilators for patients with symptomatic COPD, FEV1 less than 50% predicted and with repeated exacerbations.
Inhaled corticosteroid therapy associated with increased risk of pneumonia in several randomized clinical trials.
There is a 50-70% increasing risk of pneumonia associated with the use of ICSs in COPD.
Increased risk of osteopenia and fractures associated with long-term inhaled corticosteroids for COPD.
Meta-analysis of 11 randomized trials of inhaled corticosteroid therapy demonstrated such therapy not associated with improved survival during follow-up periods of 6 months to 3 years, and was associated wit a 34% increased in the risk of pneumonia (Drummond).
Inhaled corticosteroids may increase pneumonia in COPD patients by local airway immunosuppression.
Inhaled corticosteroid therapy associated with reduction of biomarkers of systemic inflammation.
Higher inhaled corticosteroids associated with increased pneumonia risk in a dose dependent fashion.
Combination therapy with inhaled corticosteroids and long-acting beta2 agonists (LABA), may increase the delivery of inhaled corticosteroids to the alveolar bed. which may increase the immunosuppressive effects of the former.
No pharmacological treatment and few interventions, other than smoking cessation and supplemental oxygen, have been shown to improved mortality.
Most interventions attempt to reduce complications and symptoms associated with the disease.
Inhaled corticosteroids therapies utilized to decreases pulmonary inflammation and can be administered as monotherapy or combination treatment with long acting Beta2-agonists.
Randomized controlled clinical trials have demonstrated that inhaled corticosteroids reduces the frequency of such exacerbations.
Inhaled triamcinolone (or other steroids) does not slow the rate of decline in pulmonary function, as measured by FEV1, but improves respiratory symptoms and airway reactivity and decreases the number of exacerbations and the use of health care resources.
To date no known agent alters the rate of decline of the FEV1 in patients with COPD (2008).
Only smoking cessation has altered the decline of FEV1.
The Lung Health Study found that in a randomized trial of smoking cessation in individuals with mild to moderaate COPD. cessation of smoking slowed lung function decline, and reduced death rate from any cause (Anthonisen NB).
It is assumed that smoking cessation will accrue health benefits at all stages of COPD.
Inhaled steroids not recommended for patients with mild COPD.
Inhaled corticosteroid therapy for COPD use for at least 24 weeks is associated with a significant increased risk of serious pneumonia, without a significantly increased risk of death (Singh).
In the Singh meta analysis with 16,996 patients using inhaled corticosteroids the risk ratio for pneumonia was increased by 60% , and in serious pneumonia by 70% without a significant increase in risk of pneumonia related death or overall death.
Inhaled fluticasone exerts effects on serum cortical levels that are equivalent to 10 mg a day of oral prednisone, a dose that may double the risk of pneumonia in rheumatoid arthritis patients (Wolfe).
Is associated with progressive reduction in the activity of histone deacetylases in the lungs of patients with increasing severity of COPD and histone deacetylase 2 is required by corticosteroids to switch off activated inflammatory genes.
While the risk-benefits of inhaled clinical steroids use in as much is favorable, it is not clearly so in COPD patients.
Inhaled corticosteroids may be associated with adverse effects, including oropharyngeal candidiasis, cataracts, fractures and increased risk for pneumonia.
The cessation of smoking is the only intervention that effectively slows the decline in pulmonary function in patients with COPD.
Systemic steroids are of clinical benefit in COPD exacerbation with maximum effect achieved within 2 weeks.
Roflumilast (Daliresp) is an oral phosphodiesterase-4 inhibitor that inhibits the breakdown of cyclic AMP and may improve FEV1 when taken with bronchodilators.
Roflumilast (Daliresp) reduces exacerbations treated with corticosteroids by 15-20% in severe to very severe COPD and a history of exacerbations.
Roflumilast (Daliresp) side effects include nausea diarrhea, anorexia, headache, weight loss, and alterations in sleep.
Often evaluated by a single test the FEV1.
A low body-mass index associated with an increased risk of death.
Single lung transplant can improve the quality of life and survival in selected patients with severe COPD but does not prevent progression of native lung disease.
In patients with COPD and type 2 inflammation is as indicated by elevated eosinophil counts, dupilumab is associated with few exacerbation and better lung function than placebo.