 Cerebral circulation occurs through a network of cerebral arteries and veins supplying the brain.
Cerebral circulation occurs through a network of cerebral arteries and veins supplying the brain.
The rate of cerebral blood flow in an adult human is typically 750 milliliters per minute, or about 15% of cardiac output. This equates to an average perfusion of 50 to 54 millilitres of blood per 100 grams of brain tissue per minute.
The cerebral circulatory system has safeguards that include autoregulation of the blood vessels.
The failure of these safeguards may result in a stroke.
The volume of blood in circulation is called the cerebral blood flow.
Sudden accelerations change the gravitational forces can severely impair cerebral circulation and normal functions to the point of becoming serious life-threatening conditions.
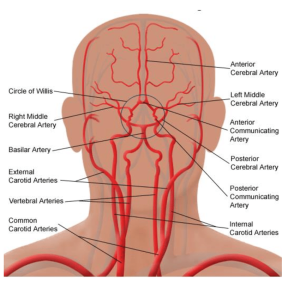
Areas of the brain are supplied by different arteries.
The major systems are divided into: an anterior circulation;the anterior cerebral artery and middle cerebral artery, and a posterior circulation.
Blood supply to the brain is normally divided into anterior and posterior segments, relating to the different arteries that supply the brain.
The two main pairs of arteries are the Internal carotid arteries which supply the anterior brain and vertebral arteries supplying the brainstem and posterior brain.
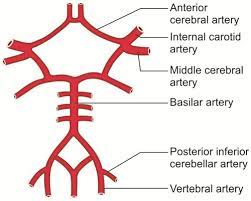
The anterior and posterior cerebral circulations are interconnected via bilateral posterior communicating arteries, part of the Circle of Willis, which provides backup circulation to the brain.
The Circle of Willis provides interconnections between the anterior and the posterior cerebral circulation along the floor of the cerebral vault, providing blood to tissues that would otherwise become ischemic.
Anterior cerebral circulation:
The anterior cerebral circulation is the blood supply to the anterior portion of the brain including eyes.
It is supplied by the following arteries:
Internal carotid arteries: the medial branches of the common carotid arteries which enter the skull, as opposed to the external carotid branches which supply the facial tissues.
The internal carotid artery branches into the anterior cerebral artery and continues to form the middle cerebral artery.
Anterior communicating artery: Connects both anterior cerebral arteries, within and along the floor of the cerebral vault.
Middle cerebral artery (MCA)
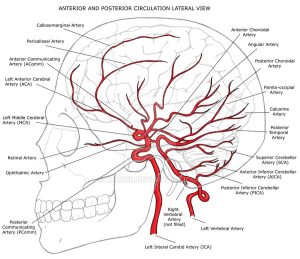
Posterior cerebral circulation
The anterior and posterior circulations meet at the Circle of Willis, which rests at the top of the brainstem.
The posterior cerebral circulation is the blood supply to the posterior portion of the brain, including the occipital lobes, cerebellum and brainstem.
It is supplied by the following arteries:
Vertebral arteries:
These smaller arteries branch from the subclavian arteries which primarily supply the shoulders, lateral chest, and arms.
Within the cranium the two vertebral arteries fuse into the basilar artery.
Posterior inferior cerebellar artery
Basilar artery: Supplies the midbrain, cerebellum, and usually branches into the posterior cerebral artery
Anterior inferior cerebellar artery (AICA)
Pontine branches
Superior cerebellar artery (SCA)
Posterior cerebral artery (PCA)
Posterior communicating artery
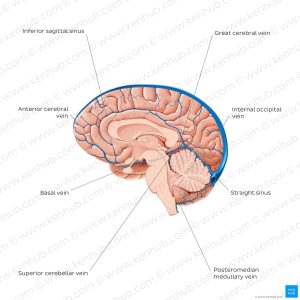
Venous drainage of the cerebrum is separated into two subdivisions: superficial and deep.
The superficial system is composed of dural venous sinuses.
The dural venous sinus walls are composed of dura mater as opposed to a traditional vein.
The dural sinuses are therefore located on the surface of the cerebrum.
The most prominent of dural sinuses is the superior sagittal sinus.
The superior sagittal sinus flows in the sagittal plane under the midline of the cerebral vault, posteriorly and inferiorly to the confluence of sinuses, where the superficial drainage joins with the sinus that primarily drains the deep venous system.
From here, two transverse sinuses bifurcate and travel laterally and inferiorly in an S-shaped curve that forms the sigmoid sinuses which go on to form the two jugular veins.
In the neck, the jugular veins parallel the upward course of the carotid arteries and drain blood into the superior vena cava.
The deep venous drainage is primarily composed of traditional veins inside the deep structures of the brain, which join behind the midbrain to form the vein of Galen.
This vein merges with the inferior sagittal sinus to form the straight sinus which then joins the superficial venous system mentioned above at the confluence of sinuses.
Dural venous sinuses direct blood outflow from cerebral veins to the internal jugular vein at the base of skull
CBF is tightly regulated to meet the brain’s metabolic demands.
Too much blood can raise intracranial pressure (ICP), which can compress and damage delicate brain tissue. Too little blood flow as in ischemia, results if blood flow to the brain is below 18 to 20 ml per 100 g per minute, and tissue death occurs if flow dips below 8 to 10 ml per 100 g per minute.
The brain tissue biochemical cascade known as the ischemic cascade is triggered when the tissue becomes ischemic, potentially resulting in damage to and the death of brain cells.
Maintaining proper CBF in patients who have conditions like shock, stroke, cerebral edema, and traumatic brain injury is necessary.
Cerebral blood flow is determined the viscosity of blood, how dilated blood vessels are, and the net pressure of the flow of blood into the brain, known as cerebral perfusion pressure, which is determined by the body’s blood pressure.
Cerebral perfusion pressure (CPP) is defined as the mean arterial pressure (MAP) minus the intracranial pressure (ICP).
The cerebral perfusion pressure In normal individuals should be above 50 mm Hg.
Intracranial pressure should not be above 15 mm Hg as ICP of 20 mm Hg is considered as intracranial hypertension.
Cerebral blood vessels are able to change the flow of blood through them by altering their diameters by cerebral autoregulation; they constrict when systemic blood pressure is raised and dilate when it is lowered.
Cerebral arterioles also constrict and dilate in response to different chemical concentrations;dilating in response to higher levels of carbon dioxide in the blood and constrict in response to lower levels of carbon dioxide.
For example, assuming a person with an arterial partial pressure of carbon dioxide (PaCO2) of 40 mmHg (normal range of 38–42 mmHg)[13] and a CBF of 50 ml per 100g per min. If the PaCO2 dips to 30 mmHg, this represents a 10 mmHg decrease from the initial value of PaCO2. Consequently, the CBF decreases by 1ml per 100g per min for each 1mmHg decrease in PaCO2, resulting in a new CBF of 40ml per 100g of brain tissue per minute. In fact,
For each 1 mmHg increase or decrease in PaCO2, between the range of 20–60 mmHg, there is a corresponding CBF change in the same direction of approximately 1–2 ml/100g/min, or 2–5% of the CBF value.
Even small alterations in respiration pattern can cause significant changes in global CBF, specially through PaCO2 variations.
CVR (cerebral vascular resistance) is controlled by four mechanisms:
Metabolic autoregulation
Pressure autoregulation
Chemical control by arterial pCO2 and pO2
Neural control
With Increased intracranial pressure (ICP) there is decreased blood perfusion of brain cells by mainly two mechanisms:
increased interstitial hydrostatic pressure that, in turn, causes a decreased driving force for capillary filtration from intracerebral blood vessels.
Increased ICP compresses cerebral arteries, causing increased cerebrovascular resistance.
The cerebral perfusion pressure is the net pressure gradient causing cerebral blood flow to the brain.
The cerebral perfusion pressure is maintained within narrow limits; too little pressure could cause brain tissue to become ischemic and too much could raise intracranial pressure.
Arterial spin labeling, phase contrast magnetic resonance imaging, and positron emission tomography (PET) are neuroimaging techniques that can be used to measure CBF.