 Multiparametric MRI (mpMRI) includes T2-weighted imaging, diffusion-weighted imaging (DWI), and dynamic contrast-enhanced (DCE) imaging, enabling precise risk stratification, targeted biopsy, and treatment planning.
Multiparametric MRI (mpMRI) includes T2-weighted imaging, diffusion-weighted imaging (DWI), and dynamic contrast-enhanced (DCE) imaging, enabling precise risk stratification, targeted biopsy, and treatment planning.
Pre-biopsy MRI is now widely established as the standard of care.
The PI-RADS v2.1 (Prostate Imaging Reporting and Data System) remains the structured reporting framework in routine use.
Men with high PSA scores may now first get a pre-biopsy MRI that helps doctors see prostate tissue in fine detail, so they can perform a more accurate biopsy — or even avoid one altogether.
The PRIME trial showed that biparametric MRI — which omits the contrast enhancement sequence — detects clinically significant prostate cancer just as well as the full multiparametric scan.
This cuts scan time from roughly 40 minutes to 20 minutes, reduces contrast toxicity, and may speed up diagnoses.
Deep learning models are being used to optimize imaging protocols and reduce acquisition times.
A 2025 systematic review confirmed consistent improvements in image quality with AI-based reconstruction techniques.
MRI-based risk-adapted screening is being studied for high-risk groups, including those with germline mutations and men with Black/African ancestry or strong family history, who carry nearly double the risk of prostate cancer.
Key Roles of Prostate MRI
1. Pre-Biopsy Triage and Cancer Detection
mpMRI before biopsy identifies clinically significant prostate cancer (Grade Group ≥2) with a sensitivity of ~93% and a negative predictive value of ~89%, compared to 48% sensitivity for standard TRUS-guided biopsy.
Approximately one in four men can safely avoid biopsy based on a negative MRI, reducing overdiagnosis of indolent disease.
However, a negative MRI does not exclude cancer — PSA density, biomarkers, and risk calculators should be considered when deciding whether to forgo biopsy.
The Prostate Imaging Reporting and Data System (PI-RADS v2.1) standardizes lesion reporting on a 1–5 scale based on the probability of clinically significant cancer.
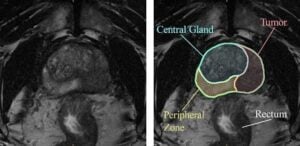
Scoring differs by prostate zone: diffusion-weighted imaging (DWI) is the dominant sequence for peripheral zone lesions, while T2-weighted imaging is dominant for transition zone lesions.
Dynamic contrast-enhanced (DCE) imaging can upgrade peripheral zone PI-RADS 3 lesions to PI-RADS 4.
MRI/ultrasound fusion-targeted biopsy is the preferred approach and significantly increases detection of clinically significant, higher-risk (Grade Group ≥3) disease while reducing detection of low-risk disease.
Most experts advocate a combined targeted plus systematic biopsy approach, as some high-grade cancers are uniquely detected by systematic sampling.
Micro-ultrasound–guided biopsy at experienced centers has been shown to be non-inferior to MRI-targeted fusion biopsy.
mpMRI is preferred over CT for local staging, as it can detect extracapsular extension (T staging) and characterize prostate cancer.
It is equivalent to CT for pelvic lymph node evaluation.
For unfavorable intermediate-risk and higher disease, PSMA-PET/CT or PET/MRI can be considered as an alternative to conventional imaging for initial staging.
mpMRI is used to risk-stratify patients considering active surveillance and to monitor for disease progression.
Combining PI-RADS category ≥4 with PSA density ≥0.15 ng/mL/cm³ decreased overdiagnosis of clinically insignificant cancer by 45% while missing only 5% of clinically significant disease.
MRI may be considered after radical prostatectomy when PSA does not fall to undetectable levels or when biochemical recurrence is detected, and after radiation therapy for rising PSA or positive DRE in candidates for additional local therapy.
mpMRI includes T2-weighted, diffusion-weighted, and dynamic contrast-enhanced sequences.
Biparametric MRI (omitting DCE) reduces scan time from 30–40 to 15–20 minutes and has shown similar diagnostic quality in some contexts, though the PRIME trial suggested multiparametric MRI may detect more cancers.