 High grade pediatric diffuse glioma incidence rate of roughly 1.8 per hundred thousand population.
High grade pediatric diffuse glioma incidence rate of roughly 1.8 per hundred thousand population.
HGPG represents approximately 15% of all intracranial neoplasm diagnosed in children and adolescents.
The incidence is highest for age groups 0–4 years at 6.1 per hundred thousand and at 15-19 years 7 per 100,000.
Prognosis of these lesions is generally poor with five year survival rates of less than 20%.
Prognosis and survival depends on age and presentation, tumor location, sex, extent of resection, histologic subtype and genomic profile.
The diagnosis is more common in females, but males typically have a higher mortality rate.
Certain inherited cancer predisposition syndromes, including neurofibromatosis type1, Li-Fraumeni syndrome, and Turcot syndrome/Lynch syndrome/Constitutional mismatch repair deficiency, are associated with increase susceptibility to pediatric diffuse high-grade gliomas.
High does of ionizing radiation is linked to pediatric brain malignancies, as well.
Ionizing radiation has greater carcinogenic potential in children as they are more radiosensitive than adults, and have more potential years of life to express risk.
The estimated risk is higher for younger children, and the estimated latency between radiation exposure and brain tumor development is 7-9 years, with meningiomas and gliomas, being the most common radiation induced tumor types.
With high-grade pediatric gliomas, the clinical presentation and symptoms depends, largely on tumor location and patient age at the time of diagnosis.
The most common symptoms include: effects of increased intracranial, pressure with headaches, nausea, vomiting, and blurred vision.
Increased intracranial pressure may be caused by growth of the tumor, edema in the brain, or blocked CSF fluid.
Other symptoms that patients may present with include: seizures, hemiparesis, monoparesis, cranial, nerve abnormalities, ataxia, sensory loss, dysphasia, aphasia, and memory impairment.
Young infants may have increasing head circumference and loss of developmental milestones.
School-aged children may experience, poor school performance, personality alterations, and fatigue.
Symptoms may occur gradually and worse over time, or be sudden such as with a seizure.
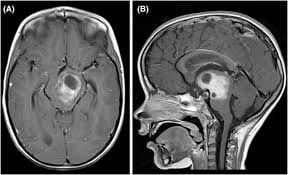
MRI is recommended for tumor diagnosis, surgical guidance, and therapeutic monitoring.
Pediatric diffuse high grade gliomas typically manifest is an infiltrative growth pattern on MRI with poorly differentiated intracranial masses within indistinct borders occupying most of one hemisphere were spread through the corpus callosum into the other hemisphere.
Basic MRI of the spine is also required to evaluate for leptomeningeal metastases.
Treatment: Management of pediatric diffuse high grade glioma depends on type of tumor, its location and size, how far it is spread, and the age and overall health of the patient.
The primary treatment includes surgery, followed by systemic therapy with or without radiation.
Goals of surgery includes safe reduction of tumor associated mass, and obtaining adequate tissue for histologic and molecular classification.
Cranial radiation may result in developmental impairment in young children and is often admitted in children less than three years of age.
Despite surgery/adjuvant therapy pediatric diffuse high grade gliomas have a poor prognosis.