 A breech presentation occurs when a fetus is positioned with its buttocks or feet facing the birth canal instead of the head.
A breech presentation occurs when a fetus is positioned with its buttocks or feet facing the birth canal instead of the head.
Breech presentation with the baby’s buttocks, feet, or both positioned to deliver first, rather than the head-cephalic presentation.
A breech presentation is common in early pregnancy, but most babies naturally turn head-down (vertex presentation) by 36–37 weeks.
Only about 3% to 4% of babies remain breech at full term.
More common at earlier gestational ages (up to ~25% at 28 weeks)
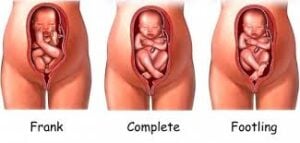
Types of Breech Positions:
The specific type is defined by the position of the baby’s legs:
Frank Breech (Extended): The most common type (50–70%). The baby’s buttocks lead, with legs pointing straight up toward the head (pike position).
Complete Breech (Flexed): The baby is “sitting” cross-legged with both hips and knees bent.
Footling Breech (Incomplete): One or both of the baby’s feet point downward and are poised to deliver first:higher cord prolapse risk
Kneeling Breech: A rare variation where the baby is positioned knees-first.
Causes and Risk Factors for breech presentation:
The cause is often unknown, several factors increase the likelihood:
Uterine/Placental Issues: Irregularly shaped uterus, fibroids, or Placenta Previa with placenta covering the cervix.
Amniotic Fluid Levels: Having too much (polyhydramnios) or too little (oligohydramnios) fluid.
Fetal Factors: Multiple gestations (twins/triplets), prematurity, or certain birth defects that limit movement.
Maternal History: Previous breech pregnancies or being in a first pregnancy.
Prematurity
Uterine anomalies (fibroids, septum)
Placenta previa
Fetal anomalies (hydrocephalus, aneuploidy)
Diagnosis Leopold’s maneuvers (firm, round head in fundus) Confirmed by ultrasound
Management and Delivery Options If a baby is still breech after 36 weeks:
External Cephalic Version (ECV): A procedure where a doctor applies firm pressure to the abdomen to manually turn the baby head-down. It is successful in roughly 50% to 60% of cases.
Planned C-Section: Most providers recommend a Cesarean delivery as the safest option for breech babies to avoid complications like head entrapment or umbilical cord prolapse.
Vaginal Breech Birth: Possible under strict criteria and with a highly skilled medical team, though it carries higher risks of birth trauma and oxygen deprivation.
Considered at some centers with experienced providers, under strict criteria-frank breech, adequate pelvis, no hyperextended fetal neck, continuous monitoring).
Complications if unmanaged Cord prolapse, especially footling Head entrapment Birth asphyxia Fetal trauma place on site with images