Spinal nerve T1
The first thoracic spinal nerve T1 is a mixed nerve, containing both somatic efferent motor and somatic afferent sensory fibers.
It originates from the spinal cord at the T1 spinal segment.
Like other nerves, the spinal nerve T1 is formed by the union of two roots:
1. Posterior (dorsal) root:
This root contains sensory fibers that carry signals from peripheral structures (innervated by the anterior and posterior rami) to the spinal cord.
These fibers enter the dorsal gray horn within the spinal cord.
2. Anterior (ventral) root:
This root consists of motor fibers originating from the anterior gray horn within the spinal cord.
These fibers transmit motor commands to peripheral muscles via the spinal nerve and its branches.
b) Mixed spinal nerve and rami
At the level of the intervertebral foramen, the anterior and posterior roots merge to form the spinal nerve T1.
This mixed nerve, containing both sensory and motor fibers, exits the intervertebral foramen between the T1 and T2 vertebrae.
Shortly after its emergence, the nerve divides into two primary rami:
1. Anterior (ventral) ramus:
This ramus continues anteriorly along the chest wall as the first intercostal nerve, within the intercostal space, providing motor and sensory innervation to the chest wall.
It also forms connections with the sympathetic trunk via the white and gray rami communicantes, which carry preganglionic and postganglionic sympathetic fibers.
The anterior ramus of the spinal nerve T1 exits the vertebral canal through the intervertebral foramen between the T1 and T2 vertebrae. A significant portion of this ramus contributes to the brachial plexus by forming a prominent communicating branch that joins with the anterior ramus of the C8 spinal nerve to create the inferior trunk of the brachial plexus.
The remaining portion of the T1 anterior ramus becomes the first intercostal nerve, which traverses the first intercostal space of the chest wall.
In this region, the nerve is part of a neurovascular bundle that includes the intercostal artery and vein.
This bundle is positioned between the internal intercostal muscle on its superficial side and the innermost intercostal muscle on its deep side, as the nerve courses along the chest wall.
The anterior ramus of spinal nerve T1, a critical contributor to the inferior trunk of the brachial plexus, provides motor innervation to several upper limb muscles.
These include:
Pectoral muscles: Pectoralis minor muscle (C8, T1) and the sternocostal head of the pectoralis major muscle (C6-T1), both supplied via the medial pectoral branch of the medial cord of the brachial plexus.
Forearm muscles (flexor side): Flexor carpi ulnaris (C7, C8, T1) via the ulnar nerve, flexor digitorum superficialis (C8, T1), via the median nerve, and flexor digitorum profundus (C8, T1); its medial half via the ulnar and lateral half via the median (anterior interosseus) nerve.
Hand muscles: T1 contributes to the innervation of intrinsic hand muscles, supplied via:
The superficial branch of the ulnar nerve (C8, T1) to palmaris brevis muscle.
The deep branch of the ulnar nerve (C8, T1) to hypothenar muscles (abductor, opponents, & flexor digiti minimi muscles), adductor pollicis, 3rd & 4th lumbricals, palmar interossei, dorsal interossei muscles.
The recurrent branch of the median nerve (C8, T1) to the thenar (abductor, opponens, & flexor pollicis brevis) muscles,
The digital branches of median nerve (C8, T1) to the 1st & 2nd lumbricals.
Thoracic wall muscles:
The remaining portion of the anterior ramus of spinal nerve T1, which continues beneath the first rib as the first intercostal nerve, provides motor innervation to important thoracic wall muscles, including:
External, internal, and innermost intercostal muscles (T1-T11).
The sensory fibers of the first intercostal nerve (T1) innervate the skin corresponding to the T1 dermatome, which is primarily located on the medial aspect of the arm.
These sensory fibers reach their target region via a cutaneous branch of the ulnar nerve, known as the medial cutaneous nerve of the arm.
Posterior (dorsal) ramus:
This ramus provides motor innervation to the deep muscles of the upper back.
It also provides sensory innervation to the skin overlying the upper back.
As a mixed nerve T1 contains both motor (somatic efferent) and sensory (somatic afferent) fibers.
The posterior ramus of the T1 is the smaller, posterior branch of the spinal nerve T1.
It innervates the deep intrinsic muscles of the back and the overlying skin, playing a vital role in spine stabilization and movement.
Once the T1 spinal nerve exits the intervertebral foramen (between the T1 and T2 vertebrae), its posterior ramus passes through the intertransverse ligament and the overlying intertransverse (intertransversarii) muscle.
It divides into lateral and medial branches:
Medial branch: Muscular branches: These innervate:
The erector spinae muscles, specifically the iliocostalis and longissimus portions.
Segmental muscles: These include the levtores costarum muscles.
Cutaneous branch: After piercing the iliocostalis muscle, the lateral branch extends to supply the skin of the back.
The medial branch travels posterolaterally before curving medially along the edge of the multifidus muscle.
Along its course it gives rise to:
Articular branches: These branches innervate the zygapophyseal joints.
Muscular branches: These branches supply the intrinsic muscles of the back, including:
Erector spinae: primarily the spinalis potion, with a minor contribution to the longissimus.
Transversospinalis group: This includes the multifidus, semispinalis (specifically the semispinalis thoracis and cervicis), and the rotatores (rotatores thoracics and cervicis).
Segmental muscles: These include the interspinales and medial slips of the intertransversarii muscles.
Cutaneous branch: After innervating the multifidus muscle, the medial branch pierces the thoracolumbar fascia and the extrinsic back muscles, to become a cutaneous branch.
ADDITIONAL STRUCTURES ASSOCIATED WITH SPINAL NERVE T1:
a) Recurrent Meningeal Nerve (Meningeal branch):
The recurrent meningeal nerve (or meningeal branch) originates from either the T1 spinal nerve or one of its rami.
This small recurrent meningeal nerve re-enters the vertebral canal through the intervertebral foramen and provides sensory innervation to:
The meninges
The annulus fibrosus of the intervertebral discs,
The vertebral bodies and periosteum,
Adjacent blood vessels.
b) Sympathetic connections:
Th3 spinal nerve T1 connects to the sympathetic trunk.
The white rami communicantes enable preganglionic sympathetic fibers to reach the sympathetic trunk, while the gray rami communicantes enable the postganglionic sympathetic fibers to reach peripheral targets such as sweat glands and blood vessels.
The T1 nerve can be affected in thoracic nerve compression, leading to symptoms such as pain or numbness radiating into the chest, upper back, and possibly the arm.
T1 thoracic nerve is crucial for upper chest, back, and arm function, providing both motor and sensory supply—especially through its contribution to the brachial plexus and intercostal muscles.
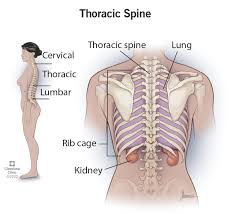
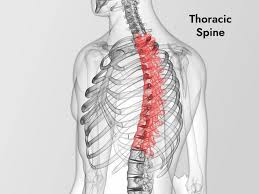
T2 is situated in the upper thoracic spine, between the cervical and lower thoracic vertebrae.
T2 is slightly larger than T1 and has facets that allow attachment to ribs, supporting upper body weight and rib movement.
The T2 spinal nerve exits just below the T2 vertebra and above T3.
T1 and T2 nerves feed into the top of the chest, also contributing to nerve supply for the arms and hands.
Motor and sensory functions from the T2 nerve include sensation and some movement in the upper chest and potentially the arm.
Injury to T2 can result in symptoms such as chest pain, heart issues including rhythm disruption, and may impact the upper chest, arms, and hands.
T2 region is less likely to cause severe disability compared to cervical injuries but can cause pain, numbness, weakness, or breathing difficulty depending on nerve impact.
T3 The T3 nerve root is a thoracic spinal nerve that emerges from below the third thoracic vertebra and primarily serves the chest wall and upper respiratory organs like the lungs.
Damage or compression of the T3 nerve can lead to pain, numbness, or tingling in the upper chest, chest wall, and potentially the back, sometimes affecting breathing.
Symptoms and sensations from the T3 nerve are associated with the area around the nipple line.
The T3 nerve root exits the spinal column between the third and fourth thoracic vertebrae.
It transmits sensory information to and from the chest wall, upper back, and the lungs and bronchial tubes.
Together with T4 and T5, it helps supply nerve networks to the chest and is involved in breathing.
Nerve distribution: The T3 nerve provides sensation to the area of the chest roughly corresponding to the third intercostal space, and the nipple line.
T3 nerve damage or compression symptoms are pain, numbness, tingling, or weakness in the upper chest or back.
Symptoms: may radiate along the nerve root, potentially causing pain that runs between the third and fourth ribs.
Difficulty breathing or chest muscle weakness, especially with certain movements.
Muscle spasms or changes in posture due to nerve irritation.
Causes of T3 nerve issues:
Inflammation: From conditions like a herniated disc or narrowing of the intervertebral foramen where the nerve exits.
Trauma: Injury to the spine can damage the nerve root.
Muscle strain: A severe strain of a muscle between the ribs can irritate the associated nerve.
T4
The fourth thoracic spinal nerve (T4) is a nerve in the upper back that provides sensation to the chest, arms, and upper abdomen, with its dermatome level generally corresponding to the nipples.
The T4 spinal nerve is a mixed nerve that carries both motor and sensory fibers.
Dysfunction or compression of this nerve can lead to a condition called T4 syndrome, which causes pain, numbness, and pins and needles in the arms, neck, and upper back, along with potential headaches and stiffness.
Severe spinal cord injuries at this level can result in a loss of function from the chest down.
Functions of the T4 nerve:
Sensory: Provides sensory innervation to the upper chest, including the area around the nipples, and the upper abdominal region.
Motor: Contributes to the motor control of muscles in the upper body.
Sympathetic: The T4 level is a key site for the sympathetic nervous system, which regulates functions like heart rate, blood pressure, and sweating.
T4 syndrome symptoms: Pain: Diffuse pain in the upper and lower arms, upper back muscles, and sometimes the neck.
Numbness: Numbness or tingling in the arms, shoulders, or palms.
Headaches: Headaches can be a symptom.
Stiffness: A feeling of stiffness in the morning or difficulty with bending and twisting movements.
Chest and ribs: Pain or radiating pain in the chest and rib area.
Reduced range of motion, weakness, and abnormal reflexes may also occur.
Causes of T4 syndrome:
Joint dysfunction: Dysfunction of the facet joints or vertebral discs of the fourth thoracic vertebra.
Traumatic injury: Sudden movements, heavy lifting, twisting, or bending can strain the joints and nerves.
Poor posture: Prolonged poor posture can lead to irritation of the nerves.
Treatment for T4 syndrome
Physical therapy: A physical therapist can recommend stretches and exercises. Medication: Over-the-counter pain relievers Ice: Applying ice to the affected area may help reduce swelling.
Severe spinal cord injury at T4 In cases of severe spinal cord injury, damage to the spinal cord at the T4 level can cause paralysis and loss of sensation from the chest down.
This type of injury can also affect breathing.
The most significant sensory function of the T4 spinal nerve is its dermatome, which is the strip of skin corresponding to the nipple line.
T4 nerve arises from the T4 segment of the spinal cord.
The T4 nerve root exits the spinal column through the intervertebral foramen, located between the T4 and T5 vertebrae.
After exiting the spinal column, the T4 nerve splits into an anterior (front) and a posterior (back) branch.
The larger anterior branch continues along the chest wall in the fourth intercostal space (the space between the fourth and fifth ribs) as the fourth intercostal nerve.
Posterior ramus: The smaller posterior branch supplies the deep muscles and skin of the back.
The T4 nerve provides motor and sensory signals to the chest wall and back.
The most clinically relevant sensory area of the T4 nerve is the T4 dermatome, which provides sensation to the area around the nipple.
This landmark is an important reference point for assessing the level of a spinal cord injury.
The T4 nerve also supplies sensation to the parietal pleura, the lining on the inside of the chest wall.
The anterior ramus of T4 provides motor innervation to the intercostal, subcostal, and transversus thoracis muscles, which aid in breathing.
Back muscles: The posterior ramus innervates the deep muscles of the back, such as the erector spinae and transversospinales muscle groups.
T4 spinal cord injury: Damage to the spinal cord at the T4 level can cause a loss of sensation and motor function from the chest down.
Individuals may experience weakness or paralysis in the trunk muscles and have impaired bowel, bladder, and temperature control.
T4 syndrome is a rare condition involving upper back and radiating upper limb pain and tingling.
It is a diagnosis of exclusion that may be linked to a dysfunction of the T4 vertebra or an effect on the sympathetic nervous system.
The T5 (fifth thoracic) nerve root is a mixed nerve that originates from the spinal cord and helps control muscles and sensation in the chest wall and helps with breathing.
The fifth thoracic nerve is a mixed nerve, containing both sensory and motor fibers, that forms from the union of the posterior (dorsal) and anterior (ventral) roots and exits the spinal canal between the T5 and T6 vertebrae.
Damage or compression of the T5 nerve root can lead to symptoms such as pain, tingling, numbness, muscle spasms, and weakness in the chest, back, shoulder, and neck.
Sensory function: It carries sensory signals from the chest wall to the spinal cord.
Motor function: It sends motor commands to muscles in the chest wall to aid in breathing.
The T5 nerve root is formed by the joining of the posterior and anterior roots within the intervertebral foramen.
Symptoms of damage or compression include pain and tenderness in the chest, back, shoulder, and neck, along with numbness, tingling, and muscle spasms.
The muscles of the chest wall and back can be affected.
Postural changes can occur as the body tries to compensate for pain and weakness.
Difficulty bending, twisting, or turning the body may occur.
Causes of T5 nerve root issues Herniated discs Degenerative disc disease Bone spurs Spinal stenosis Osteoarthritis in the spine Spinal injuries Trauma or muscle spasm
T6
The sixth thoracic spinal nerve (T6) is a mixed nerve that carries both motor and sensory information to and from the trunk.
Originating from the spinal cord at the T6 level, it is a key component of the nervous system’s control over the mid-chest and abdominal region.
T6 is formed by the joining of two roots:
Dorsal (posterior) root: Contains sensory nerve fibers that transmit signals from the skin and other structures back to the spinal cord.
Ventral (anterior) root: Contains motor nerve fibers that send commands from the spinal cord to muscles.
After the two roots merge to form the spinal nerve, it exits the spinal canal through an opening called the intervertebral foramen.
It then divides into branches that supply different parts of the body.
Motor control of T6-Supplies motor function to the intercostal muscles between the ribs and the muscles of the chest and abdomen.
Works with other thoracic nerves to provide stability to the chest and abdomen, and an injury can affect core muscles important for posture and balance.
Sensory fibers from the T6 nerve innervate the skin of the chest at the level of the xiphoid process, and provides sensation to deeper structures, including the parietal pleura.
The T6 nerve is involved with the sympathetic nervous system, influencing involuntary functions that can affect the digestive system, such as stomach upset, indigestion, and heartburn.
T6 nerve compression or irritation can cause a condition called thoracic radiculopathy.
Symptoms can include:
Radiating pain: A sharp, burning, or shooting pain that wraps around the chest or abdomen in a “band-like” pattern.
Numbness and tingling: Abnormal sensations in the ribs, abdomen, or chest.
Muscle weakness and spasms: Weakness in the core or other affected muscles.
Loss of sensation: Can include an abnormal sensitivity to light touch or a loss of feeling in the affected area.
Damage to the spinal cord at the T6 level is more serious than a simple nerve compression, as it affects all nerves below that point.
A T6 spinal cord injury can cause paraplegia and other major complications:
Impaired walking and balance with damage to the core muscles can make it difficult to sit upright and lead to walking impairments.
Bowel and bladder dysfunction
Autonomic dysreflexia: involves a sudden, dangerous spike in blood pressure in response to a stimulus below the level of injury.
Pressure sores:
T7
T7 nerve, which provides both motor and sensory innervation to the mid-chest, mid-back, and upper abdomen.
The seventh intercostal nerve and its anterior ramus is responsible for sensations and muscle control in these areas, which can include the muscles in the abdominal wall and the skin over the mid-to-upper abdomen.
Damage to this nerve can cause symptoms like pain, tingling, or numbness in a band-like pattern around the torso.
The T7 nerve is a mixed nerve, carrying both motor and sensory information.
It controls muscles in the chest and upper abdomen.
Sensory: It provides sensation to the skin of the mid-chest, mid-back, and upper abdomen.
Location: It originates from the spinal cord at the T7-T8 level and exits the spinal canal.
Its anterior ramus (the seventh intercostal nerve) travels along the seventh rib and then continues into the abdominal wall behind the rib cage.
Nerve damage symptoms:
Pain: T7 nerve damage, also called thoracic radiculopathy, can cause sharp, dull, or radiating pain in the mid-back, chest, or upper abdomen.
Numbness and tingling in the skin of the affected area.
Muscle weakness: In some cases, nerve damage can lead to weakness in the associated muscles, though this is less common than pain or sensory changes.
Abdominal discomfort: Irritation of the T7 nerve can cause abdominal pain that is sometimes mistaken for digestive issues.
The T7 nerve can be involved in conditions affecting the thoracic spine, such as a herniated disc.
Its role in innervating both the chest and abdominal walls means that injury can cause symptoms in both areas.
T8
The T8 nerve is the eighth thoracic spinal nerve, originating from below the eighth thoracic vertebra.
It serves the mid-abdominal region, supplying sensory and motor signals to the chest and abdominal wall muscles.
Damage or compression can lead to pain, numbness, tingling, and muscle weakness in the corresponding area of the body.
T8 nerve emerges from the spinal column below the T8 vertebra.
Dermatome: The T8 nerve’s sensory dermatome is located at the level of the lower edges of the ribcage, extending to the upper abdomen. Intercostal nerve: Its larger branch, the eighth intercostal nerve, runs within the eighth rib’s costal groove and continues into the abdominal wall.
T8 helps control the muscles of the chest and abdomen, and provides sensation to this area. If the T8 nerve root is compressed or irritated, it can cause sharp, radiating pain around the chest or abdomen.
Numbness or tingling in the torso can occur.
Muscle weakness: In some cases, muscle weakness can result from nerve compression.
T9
The T9 spinal nerve is the ninth thoracic spinal nerve, originating below the T9 vertebra.
It plays a role in the function of the lower thoracic and upper abdominal regions, including supplying nerves to the abdomen, muscles like the external oblique and rectus abdominis, and innervating deeper structures and the diaphragm.
Nerve damage can result in pain, numbness, or weakness in the associated areas.
The T9 nerve and other lower thoracic nerves innervate muscles of the abdominal wall, such as the transversus abdominis, internal oblique, and rectus abdominis.
The T9 nerve is associated with the greater splanchnic nerve, which influences various organs.
Sympathetic signals from T9 can affect the liver, pancreas, and adrenal medulla.
It sends sensory twigs to the adjacent diaphragm and pleura.
The T9 nerve contributes to the sensory and motor functions of the lower back and abdomen.
Persistent pain in the mid-back or abdominal area is a common symptom.
Sensory changes of numbness or tingling in the areas associated with the T9 nerve, such as the rib cage and abdomen may be experienced
Difficulty moving or weakness in the muscles of the abdominal wall can occur.
In more severe cases, damage can impact the bowel and bladder.
T10
The T10 nerve root is the tenth thoracic spinal nerve, a mixed nerve that carries both sensory and motor fibers.
It exits the spinal canal between the T10 and T11 vertebrae.
The T10 nerve root provides sensation to the skin at the level of the umbilicus.
Motor It innervates the muscles of the lower abdominal wall, specifically portions of the external oblique, internal oblique, and transversus abdominis muscles, along with intercostal muscles and deep back muscles-erector spinae and transversospinales groups.
It connects to the sympathetic trunk via rami communicantes, carrying fibers that regulate functions like sweat glands and blood vessels in the periphery, and may be involved with kidney function.
Compression or irritation of the T10 nerve root/thoracic radiculopathy, can cause pain, numbness, tingling, or weakness in its distribution areas.
Pain from T10 nerve root issues is often felt in the umbilical region.
A lesion at the T9 or T10 nerve roots can result in the paralysis of the lower abdominal muscles, while sparing the upper ones.
When the patient tries to flex their abdominal wall, the umbilicus may move upward, a clinical sign known as the Beevor sign.
Complete damage to the spinal cord at the T10 level can result in paraplegia and loss of sensation and muscle control in the lower abdomen and below.
T11
The thoracic T11 spinal nerve is a mixed nerve, meaning it contains both motor (efferent) and sensory (afferent) fibers.
It provides motor and sensory innervation to parts of the lower back, the abdominal wall, and the skin in the area just below the umbilicus.
The T11 spinal nerve originates from the spinal cord at the T11 segment and exits between the T11 and T12 vertebrae.
It then divides into an anterior ramus (eleventh intercostal nerve) and a posterior ramus.
The T11 nerve supplies motor function to muscles in the thoracic and abdominal walls, such as the intercostal, abdominal oblique, and rectus abdominis muscles.
Its posterior ramus innervates the deep muscles of the back, like the erector spinae and transversospinales muscles, which are important for stabilizing the spine.
T11 provides sensation to the T11 dermatome, which is the skin just below the umbilicus.
It also provides sensory input from deeper structures, including the pleura and peritoneum, as well as the skin and joints of the back at the T11/T12 level.
Damage to the T11 nerve can lead to pain, numbness, tingling, or weakness in the lower chest, upper abdomen, and lower back region.
T12
The T12 spinal nerve is the twelfth and final mixed nerve of the thoracic region, responsible for providing motor innervation to the lower abdominal and deep back muscles and sensory innervation to the skin of the lower abdomen and back.
The T12 spinal nerve originates from the T12 spinal cord segment.
The mixed nerve exits the vertebral canal through the intervertebral foramen located between the T12 and L1 vertebrae.
Shortly after exiting, it divides into two primary rami: Posterior (dorsal) ramus: This smaller branch travels posteriorly to innervate the deep, intrinsic muscles of the lower back and the skin overlying this region.
Anterior (ventral) ramus: This larger branch is also known as the subcostal nerve because it runs inferior to the twelfth rib.
It continues along the abdominal wall, providing innervation to various abdominal muscles.
It may also send fibers to the L1 spinal nerve, contributing to the lumbar plexus.
Anterior Ramus (Subcostal Nerve): External oblique, internal oblique, transversus abdominis, rectus abdominis, and quadratus lumborum muscles.
Skin of the lower abdomen (above the inguinal crease, including the pubic region) and the parietal peritoneum.
Posterior Ramus Deep back muscles: erector spinae (iliocostalis, longissimus, spinalis portions), transversospinalis muscles (multifidus, semispinalis, rotatores), and segmental muscles.
Skin of the lower back and the zygapophyseal joints between the T12 and L1 vertebrae.
Damage or compression of the T12 spinal nerve or spinal cord segment can cause a variety of symptoms, including:
Pain: Sharp, shooting, or searing pain in the mid-back, side of the body, or abdomen.
Sensory deficits: Numbness or altered sensation in the skin regions of the T12 dermatome.
Motor deficits: Weakness in the abdominal and deep back muscles, which can affect trunk stability, posture, and in severe cases, contribute to difficulty standing or walking.
Bowel and Bladder Issues: Severe spinal cord compression at the T12 level can potentially impact bowel and bladder control functions.
Conditions that can affect the T12 nerve include disc herniation, spinal stenosis, fractures, degenerative disc disease, and nerve compression from bone spurs or trauma.