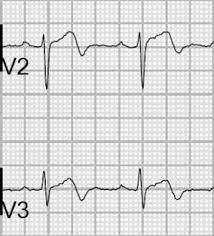
 Biphasic T waves in leads V2 and V3.
Biphasic T waves in leads V2 and V3.
Wellens’ syndrome is an electrocardiographic manifestation of critical proximal left anterior descending (LAD) coronary artery stenosis in patients with unstable angina.
It is characterized by symmetrical, often deep (>2 mm), T wave inversions in the anterior precordial leads.
A less common variant is biphasic T wave inversions in the same leads.
First described in a subgroup of patients with unstable angina, identified in 14% of patients at presentation and 60% of patients within the first 24 hours.
The presence of Wellens’ syndrome carries significant diagnostic and prognostic value, with more than 50% stenosis of the left anterior descending artery with complete or near-complete occlusion in 59%.
In the original Wellens’ study 75% of those with the typical syndrome manifestations had an anterior myocardial infarction.
Wellens’ sign is rarely seen with Takotsubo cardiomyopathy or stress cardiomyopathy.
Diagnostic criteria: Progressive symmetrical deep T wave inversion in leads V2 and V3
Slope of inverted T waves generally at 60°-90°
Little or no cardiac marker elevation
Discrete or no ST segment elevation
No loss of precordial R waves.
Is an electrocardiographic manifestation of critical proximal left anterior descending (LAD) coronary artery stenosis in patients with unstable angina.
Chararacterized by symmetrical, often deep >2mm, T wave inversions in the anterior precordial leads.
A less common variant is biphasic T wave inversions in the same leads.
This syndrome is identified in 14% of patients with unstable angina at presentation and 60% of patients within the first 24 hours.
Patients with characteristic findings have more than 50% stenosis of the left anterior descending artery with complete or near-complete occlusion in 59%.
Wellens’ sign may rarely be seen with presentation of Takotsubo or stress cardiomyopathy.
When findings are obtained in a chest pain free interval it may herald development of an acute myocardial infarction.
Wellend syndrome is found in 5.7% of patients with acute coronary syndrome and 8.8% of patients with non-ST elevation myocardial infarction who undergo coronary angiography.
Among patients with NSTEMI those with Wellend syndrome and less likely to have a history of coronary heart disease or a previous percutaneous coronary intervention than individuals without Wellens.
Criteria:
Progressive symmetrical deep T wave inversion in leads V2 and V3
Slope of inverted T waves generally at 60°-90°
Little or no cardiac marker elevation
Discrete or no ST segment elevation
No loss of precordial R waves.
Pattern abnormal during chest-pain free periods
Patients with Wellens syndrome who want to go coronary angiography have a six month cardiovascular mortality rate of about 5%.