

Trichophagia is most often associated with trichotillomania, which is a body focused, repetitive behavior disorder of obsessive compulsive nature.
Trichotillomania has a worldwide prevalence of one to 2% and is characterized by recurrent, pulling out of the hair with result in hair loss.
Trichotillomania is associated with repeated attempts to stop the behavior and is associated with distress or impairment and functioning.
Recurrent pulling out of one’s hair with noticeable hair loss.
Trichotillomania (TTM), also called hair-pulling disorder.
Repetitive hair pulling, leading to noticeable hair loss and functional impairment.
Approximately 4% of the population is affected by TTM.
It is seven times more prevalent in children as in adults.
Majority of cases occurring between ages 4 and 17 years.
Many individuals do not seek help.
88% to 94% are female.
Medical complications include:skin irritations at the hair-pulling site, infections, and repetitive-use hand injuries.
Some patients ingest hairs risking dental and serious gastrointestinal complications caused by trichobezoars.
Associated with significant distress and impairment in emotional and social interrelationships.
Comorbidity is very common and includes anxiety disorders, mood disorders, substance use disorders, eating disorders, and personality disorders.
The scalp, eyebrows, and eyelashes are the most common areas for hair pulling.
Rarely patients pull hair from the legs, armpits, and pubic region.
Approximately 10 to 30% of patients ingest the hair.
Neuroimaging studies of patients suggest abnormalities in neural regions involved in cognition such as the frontal cortex, and affect regulation by alteration in the amygdala-hippocampal area, and habit learning with putamen changes.
Neuroimaging studies of patients suggest abnormalities in neural regions involved in cognition such as the frontal cortex, and affect regulation by alteration in the amygdala-hippocampal area, and habit learning with putamen changes.
May be associated with altered reward processing within the central nervous system.
In the DSM-5 it is categorized under obsessive-compulsive and related disorders.
Obsessive-compulsive disorder is commonly misdiagnosed for TTM, and often coexist and aggregate in the same family.
Hair pulling may be sporadic or sustained.
Stress may increase hair pulling but the process may occur during periods of relaxation.
Estimated that 2.5% of the population have engaged in such behavior.
Trichotillomania is most commonly seen in women and girls and typically begins in early adolescence.
Obsessive, compulsive disorder, attention deficit, hyperactivity disorder, and depression or common among patients with trichotillomania.
Usually associated with a psychiatric disorder.
Usually affects young women with the tendency of pulling out their own hair and eating it.
50 to 70% of patients with trichotillomania have oral ritualistic behaviors associated with hair, pulling such as rubbing hair across lips or biting the roots of hair.
The prevalence of trichophagia among patients with trichotillomania ranges from 5 to 20%.
Trichotillomania is associated with shame, embarrassment, and impedes patient’s willingness to disclose such behavior.
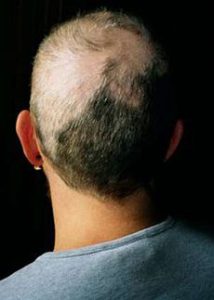
Signs of trichotillomania include patches of hair loss, hairs a various lengths andgrowth stages, redness, or inflammation of the scalp as a result of frequent hair pulling or manipulation.
Hair pulling in patients with trichotillomania is a self regulation mechanism, including mood, affect, sensory experience, environmental stresses, or negative thought patterns.
Among patients with triage the prevalence of trichobezoar is approximately one percent.
Trichotillomania patients report relief from tension along with the positive satisfaction type feeling when pulling their hair.
Trichotillomania is a chronic condition that waxes and wains overtime.
There are no medications approved for the treatment of trichotillomania.
N-acetylcysteine a natural supplement with antioxidant properties may be beneficial.
Selective serotonin uptake inhibitors have not shown benefit.
Standard behavioral therapy includes habit reversal therapy with stimulus control.
Most common symptoms of trichobezoar are abdominal pain, vomiting, gastrointestinal bleeding.
May cause anemia and hematemesis.
Can extend from the stomach into the duodenum and small intestine, and can reach the colon on rare occasions and is known as Rapunzel syndrome.
In the small intestine bezoars can fragment and dislocate and can lead to an ileus.
Options for treatment include endoscopic removal of the hair ball, open surgery or laparoscopic intervention.