 See ((
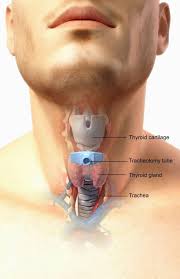
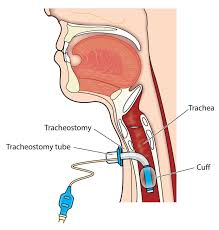
See ((Surgical procedure utilized to replace an endotracheal tube in patients expected to need long-term entilatiom, by opening a direct airway through an incision in the trachea and providing a stoma to serve as an airway or as a site for a tracheostomy tube to be inserted.
Surgical and percutaneous techniques are widely used in current surgical practice.
Advantages over prolonged endotracheal tubes include the prevention of ventilator associated pneumonia, earlier weaning from ventilator support, and decrease use of sedation.
Provides access to the airway that is more stable, and better tolerated than endotracheal tubes, and it facilitates pulmonary secretions, oral feedings and allows more patient communication.
Consensus is that the procedure should be performed after 3 weeks of endotracheal intubation (Plummer AL).
Acutely, indications for tracheotomy include facial trauma, head and neck cancers, large congenital tumors of the head and neck, angioedema and inflammation of the head and neck, and failed intubation.
In the chronic setting, indications for tracheotomy include the need for long-term mechanical ventilation and tracheal toilet.
Rarely, the procedure may be indicated as a treatment for severe obstructive sleep apnea in patients intolerant of CPAP therapy.
Procedure on children is more difficult because of their smaller size, and in patients with a short neck, are obese and have large thyroid glands.
To limit the risk of damage to the recurrent laryngeal nervesthe procedure is performed as high in the trachea as possible.
Generally performed under general anesthesia.
Complications include hemorrhage, loss of airway, subcutaneous emphysema, wound infections, fracture of tracheal rings, improper placement of the tracheotomy tube, and bronchospasm.
Bedside percutaneous tracheostomy reported overall complication rates of 10–15% and a mortality of 0%.
Tracheal ring fractures are common complication of percutaneous tracheotomy, but of unknown long-term significance.
Tracheotomy performed earlier than 3 weeks may be associated with quicker weaning from mechanical ventilation, but this has not been the experience in randomized controlled trials.
Tracheotomy within 2 days of hospital admission decreases mortality rate, incidence of pneumonia, and length of ICU stay compared with the procedure after 14-16 daysof endotracheal intubation (Rumbak MJ).
In a study comparing tracheotomy within 4 days following intubation compared to waiting at least 14 days: no difference was noted in mortality, duration of mechanical ventilation, length of ICU stay and incidence of infections (Blot F).
In a randomized trial comparing early tracheotomy, after 6-8 days of intubation, compared to late tracheotomy, days 13-15, in 600 patients without pneumonia: no statistical improvement was noted in incidence of ventilator associated pneumonia (T2241agni PP).
Percutaneous techniques for the placement of tracheotomy has increased bedside performance of the procedure.
The rates and timing for the procedure has wide variation among ICU’s.