 T1-weighted imaging is an MRI sequence that provides anatomical detail and is primarily used to detect hemorrhage, post-biopsy changes, and to help distinguish between different tissue types, but it is not central to prostate cancer detection or characterization in either biparametric or multiparametric MRI protocols.
T1-weighted imaging is an MRI sequence that provides anatomical detail and is primarily used to detect hemorrhage, post-biopsy changes, and to help distinguish between different tissue types, but it is not central to prostate cancer detection or characterization in either biparametric or multiparametric MRI protocols.
In the context of prostate cancer evaluation, multiparametric MRI (mpMRI) typically consists of T2-weighted, diffusion-weighted, and dynamic contrast-enhanced (DCE) sequences for cancer detection and staging, as recommended by the National Comprehensive Cancer Network and reflected in major clinical trials.
Biparametric MRI (bpMRI) omits the DCE sequence and relies on T2-weighted and diffusion-weighted imaging for lesion detection and risk stratification.
T1-weighted imaging is routinely acquired in both bpMRI and mpMRI protocols, but its role is supportive rather than diagnostic for prostate cancer. It is mainly used to:
Identify post-biopsy hemorrhage, which can confound interpretation of cancer-suspicious lesions on other sequences.
Exclude non-tumor pathology (e.g., cysts, calcifications).
Provide anatomical reference for fusion with other imaging modalities or for guiding targeted biopsy.
T1-weighted imaging does not contribute directly to the PI-RADS scoring system or to the identification of clinically significant prostate cancer.
The diagnostic accuracy and cancer detection rates in bpMRI and mpMRI are determined by T2-weighted and diffusion-weighted imaging (and DCE in mpMRI), not by T1-weighted imaging.
T1-weighted imaging is a standard anatomical sequence used for context and artifact detection, but it is not a core component for prostate cancer detection in bpMRI or mpMRI protocols.
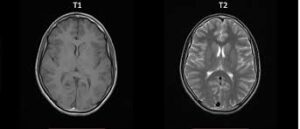
T1-weighted imaging (T1WI), also known as spin-lattice relaxation imaging, is one of the fundamental pulse sequences in magnetic resonance imaging (MRI).
It highlights differences in the T1 relaxation time—the time it takes for protons in tissues to realign with the magnetic field after excitation—providing excellent anatomical detail, particularly for structures with high fat content.
Short Repetition Time (TR): Typically 300–700 ms, allowing tissues with short T1 (e.g., fat) to recover magnetization fully before the next excitation, while longer-T1 tissues (e.g., water) recover less.
Short Echo Time (TE): Usually <30 ms, minimizing T2* decay effects so the image primarily reflects T1 differences rather than T2 (transverse relaxation).
These settings maximize contrast based on T1 properties, suppressing T2 contributions for cleaner anatomy visualization.
Signal Intensities on T1-Weighted Images
Tissues appear with characteristic brightness based on their T1 relaxation rates (shorter T1 = brighter signal):
Fat: Bright (white) due to short T1. Water/CSF: Dark (black). White Matter: Intermediate to bright (brighter than gray matter). Gray Matter: Intermediate. Muscle: Dark gray. Air/Bone: Very dark (signal void).
With gadolinium contrast, enhancing lesions appear bright due to shortened T1 in areas of blood-brain barrier breakdown.
T1WI is ideal for: Anatomical Mapping: Excellent for delineating normal structures like the brain, musculoskeletal system, and fetal organs.
Contrast-Enhanced Studies: Post-gadolinium T1WI detects tumors, infections, or inflammation by highlighting vascularized tissues.
Neurology: Identifies hemorrhage (subacute stages appear bright) and evaluates pituitary or thyroid glands.
Musculoskeletal: Assesses bone marrow, cartilage, and fat planes.
T1WI excels in anatomy, T2WI highlights edema or pathology via water signal.