 It is designed to replace the conventional 2D mammogram, offering several clinical and practical benefits:
It is designed to replace the conventional 2D mammogram, offering several clinical and practical benefits:
Lower Radiation Dose: Traditionally, a 3D mammogram was combined with a standard 2D mammogram, requiring two separate X-ray exposures.
Because synthetic mammography generates a 2D view from the 3D data, it requires only a single X-ray exposure, significantly reducing the patient’s radiation dose.
By eliminating the need for a second, separate 2D X-ray, the overall scan duration is shorter, improving the screening workflow and patient comfort.
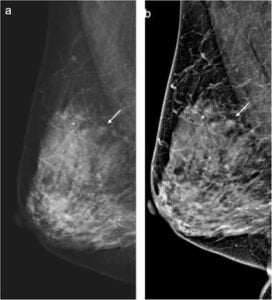
Improved Visualization: The computer algorithm used to create the image can intentionally highlight specific features—such as microcalcifications or architectural distortions—making potential abnormalities easier to spot.
During a 3D mammogram, the X-ray arm moves in an arc over the breast, capturing multiple thin, layered images, like slices of bread, Instead of performing an extra, separate 2D exposure, radiologic software compiles these 3D “slices” and flattens them into a single 2D synthetic image.
This synthetic view closely resembles a traditional 2D mammogram, allowing radiologists to easily compare the new scan against the patient’s older 2D historical records.
Advantages Decreased radiation exposure-May produce minor visual artifacts (such as blurring or bright bands
Shorter appointment/acquisition times
Better detection rates and fewer unnecessary callbacks (when paired with 3D mammography)
Synthetic mammograms are FDA-approved as a substitute for traditional 2D mammograms during a combined 2D/3D screening exam, but are not intended to be used as a 2D standalone screening tool.
Digital breast tomosynthesis plus synthetic mammography depicted more cancers and found a lower number of stage II cancers at repeat screening compared with full-field digital mammography (FFDM).
The strategy of pairing DBT, or 3D mammography, with the 2D technique of synthetic mammography is viable for screening programs due to its ability to reduce radiation exposure.
The cancer detection rate was found to be higher for repeat screening with DBT plus synthetic mammography (8.1 per 1000 women screened) compared with the control group with FFDM (4.5 per 1000 women screened. Place on site synthetic mammography