 New or recurrent strokes affect about 795,000 people in the US each year: about 700,000 are acute ischemic strokes.
New or recurrent strokes affect about 795,000 people in the US each year: about 700,000 are acute ischemic strokes.
About 23% of strokes are recurrent.
An incidence rate of 670-970 per 100,000 patients per year.
A reduction in stroke risk that has occurred has resulted from lifestyle changes such as smoking cessation, more regular exercise, advancement in the treatment of hypertension, hyperlipidemia, and better control of vascular complications of diabetes and the use of antiplatelet drugs.
While there has been an overall decline of stroke incidence in high-income countries in the 21st century, incidence at younger ages, usually defined as less than 55 years, appears to be increasing in the US and some other countries.
Antiplatelet drugs are estimated to have reduced the relative risk of stroke by approximately 25%, or the absolute risk by 3.6 percentage points in a metaanalysis over a period of two years.
Fifth leading cause of death in the US.
Accounts for nearly 150,000 deaths per year and a prevalence of about 2.5% or 7 million Americans.
Despite the use of secondary preventive strategies, 5.1% of patients with ischemic stroke or TIA have a recurrent stroke within one year.
Five years after a minor stroke or TIA, approximately 22% of persons who had survived the event are dead or disabled.
Stroke is the third leading cause of death for women and the leading cause of disability in the US.
The leading cause of hospitalization for neurologic disease.
15 million strokes occur annually worldwide.
Someone in the US has a stroke every 40 seconds, with over 75% of these cases being new or first strokes.
Global burden of stroke has been increasing.
Misdiagnosis rate is approximately 10%.
The global lifetime risk of stroke from the age of 25 years on which was approximately 25% in 2016, among both men and women.
There is particularly high lifetime risk of stroke in East Asia, Central Europe, and Eastern Europe.
Approximately one in seven individuals with a malignant neoplasm experience a stroke.
Conversely, 10% of hospitalized patients with stroke, have a comorbid cancer.
Patients with active cancer and ischemic stroke, have notoriously high rates of recurrent strokes and thromboembolic events: approximately 37% of patients with cancer will have a recurrent thromboembolic event at six months after their initial stroke.
The consequences of recurrent strokes are often more severe and disabling than the index event.
Account for almost 5% of all disability-adjusted life-years and 10% of all deaths worldwide.
More than 75% of deaths from stroke and more than 80% of disability-adjusted life-years occur in low income and middle income countries.
Approximately 10-15% of all strokes occur in young adults aged 18-49 years.
137,000 patients with stroke die of stroke complications.
600,000 strokes occur for the first time each year.
185,000 strokes per year are recurrent events.
About 77% of strokes are first events.
53.5% of strokes occur in women.
In 2010 women accounted for about 60% of stroke related deaths.
An estimated 3.8 million women and 3 million men are living in United States after having had a stroke.
One stroke every 40 seconds in the United States with 600,000 of the 795,000 strokes being new.
On average every 4 minutes someone dies of stroke.
Stroke is the leading cause of long term disability in adults.
65% of stroke survivors have some degree of impairment.
Annual cost of stroke care exceeds $70 billion.
One of every three deaths in United States is attributable to stroke, and the financial cost was estimate on 2010 both direct indirect costs to be about $315.4 billion.
90% of all strokes are ischemic and of those 10% are caused by large artery stenosis.
10% of strokes are due to intra cerebral hemorrhage and 3% due to subarachnoid hemorrhage.
Atherosclerotic narrowing of the internal carotid artery’s is an important cause of stroke.
Occurs in 1.3% of the US Medicare beneficiaries annually.
Cardiorespiratory fitness has an inverse relationship with stroke morbidity and mortality in white but not in blacks.
Blacks have a higher stroke incidence and mortality than do whites in the US.
One of every 18 deaths in 2007 due to stroke.
More than 137,000 die annually of stroke in the US.
Third leading cause of death in the U.S.
Stroke occurs more often in women than men.
Stroke is the third leading cause of death in women.
Stroke is the fifth leading cause of death in men.
One third of strokes represented recurrent events.
CDC reported in 2005 2.6% of US adults had a history of stroke.
Approximately 15,000,000 people worldwide have a stroke each year.
More than 6.0 million deaths per year worldwide.
Projected in 2010 to have both direct and and direct costs totals 73.7 billion dollars.
Approximately half of stroke deaths occur before hospital admission.
Second leading cause of death worldwide.
Poststroke epilepsy occurs in 2 to 4% of patients with stroke.
Mainly affects elderly, but 10% occur in individuals younger than 50 years.
Is a preventable disease.
Incidence varies by sex and ethnic group.
Up to 14% of all strokes occur in children and young adults.
The incidence rates of strokes in young adults are 10-23 ischemic strokes for 100,000 young adults aged 18-50 years and 3-9 hemorrhagic strokes per 100,000 young adults.
Rates of strokes decreased in US. by approximately 40% from 1988 to 2008.
Decrease in strokes parallels increasing use of antihypertensive and statin medications.
Higher levels of vWF are more common amongst people who have had ischemic stroke for the first time.
Diagnosis in young individuals underrecognized and often misdiagnosed, particularly those less than 35 years of age and those with impaired posterior circulation.
Prevalence higher among older persons, American Indians/Alaska natives, blacks and persons with lower levels of education.
Median survival times after a first stroke 13.1 years for men and 7.8 years for women at 55-64 years of age, and 6.2 years for men and 7.7 years for women at 65-74 years of age.
Prevalence and patients 20 years or older approximately 2.9% across US population, with significant regional, age, sex and racial differences.
The age-adjusted incidence of first ischemic stroke is more than twice as high in black as in white patients.
The black versus white incidences rate ratio is highest at midlife and decreases thereafter.
The prevalence of hypertension is higher in blacks and the control of hypertension in blacks is relatively poor, and when compared with whites they are more susceptible to stroke, given the same level of elevated blood pressure (Howard G et al).
Coronary Artery Risk Development in Young Adults study: Stroke is 4 times as common in Black middle-aged adults than in White middle-aged adults.
The incidence rate for stroke was 29 per 100,000 person-years for White adults and 120 per 100,000 person-years for Black adults.
Seventh most common reason for hospitalization in the US.
Majority of patients survive a stroke, making it a disorder a major source of human disability.
Thirty day mortality has decreased over time for ischemic and hemorrhagic strokes.
20-30% of stroke survivors have poor outcomes up to 10 years after stroke.
Fever with stroke associated with poor outcomes.
Fever has been demonstrated to occur in 90% of patients with stroke within seven days and it is associated with secondary brain injury and worse outcomes.
For each 1°C to increase in temperature, the odds of poor outcome increased by 2.2
Short term mortality at odds and increase by 2.2 in a patient with the ischemic stroke experience his fever within 24 hours.
Subarachnoid hemorrhage and intercerebral hemorrhage fever is correlated with worse outcomes, especially when it occurs within the first 72 hours.
Between 50-70% of stroke survivors regain functional independence, 15-30% are permanently disabled, and 20% require institutional care at 3 months.
In younger stroke victims the prognosis is more benign than in the elderly, with a lower short term mortality.
Among adults 18-50 years the 20 year mortality following acute stroke is relatively high compared to age and sex matched control groups ( Rutten-Jacobs LCA et al).
In the above study excess mortality was highest in the youngest group indicating cardio embolic stroke is the most important predictor of mortality.
Excess mortality in the above study was attributable to vascular causes, even decades after stroke, suggesting the the underlying vascular disease that caused the stroke at young age increases vascular risk throughout their lives.
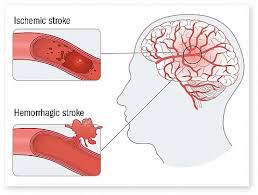
In the US 87% of strokes are ischemic and 13% hemorrhagic (10% intracerebral and 3% subarachnoid hemorrhage).(Lloyd-Jones).
With modern techniques the etiology can be determined in nearly 90% of cases.
In other countries the rate of hemorrhagic strokes may be higher, up to 25-60% (Brainin M, Durai Pandian J).
Causes and risk factors for ischemic stroke and young adults and adolescents include: large vessel atherosclerosis. 2-11%, small vessel disease 7-14%, cardiac embolism 20-47% and other causes 20-34% and multiple causes 2-3%.
Risk factors include: hypertension, atrial fibrillation, diabetes and smoking
A confirmed diagnosis of atrial fibrillation was the presumed cause of strokes in 12% of cases.
Atherosclerotic stenosis of the major intracranial arteries, which include the carotid, middle cerebral, vertebral, and basilar arteries is one of the most common causes of stroke and is associated with a higher risk of recurrence.
In Warfarin Aspirin Symptomatic Intracranial Disease trial aspirin was as effective and safer than Warfarin for preventing stroke in patients with symptomatic intracranial stenosis, however neither therapy was particularly effective in the most severely stenotic lesions.
Headache, neck stiffness, vomiting and coma are more common in hemorrhagic strokes.
Previous transient ischemic attacks, atrial fibrillation, and the presence of atherosclerosis factors are more common in ischemic strokes.
All patients with a new stroke must undergo CT scan of the brain to differentiate intracerebral hemorrhage from ischemia.
Both types of stroke cause the abrupt dysfunction of nervous system function with the development of hemiparesis, hemisensory loss, aphasia, ophthalomoplegia, and visual field cuts.
Cerebral hemorrhage in addition to the above causes displacement and compression of adjacent brain with increased intracranial pressure and dissection into the subarachnoid space: these changes can cause additional symptoms of headache, increased neurologic deterioration from continued bleeding, vomiting from increased intracranial pressure, neck stiffness by meningeal irritation, bilateral Babinski signs, and coma. .
Third cause of mortality and number one cause of disability in adults in the U.S.
Prevalence in young adults between 5 and 8 per 1,000 subjects with and incidence higher in men.
80% ischemic.
Among older patients the recent diagnosis of atrial fibrillation is associated with increased risk for stroke in women rather than men regardless of warfarin use (Tsadok MA et al).
This suggests that current day anticoagulant management to prevent stroke in older women may not be adequate.
Higher risk of stroke in women vs men with AF.
Stroke risks unique to women include hormone exposure, reproductive health, pregnancy, and childbirth.
Risk factors for stroke found in both males and females tend to be stronger in women and include: hypertension, migraine with aura, atrial fibrillation, diabetes, depression, and emotional distress.
Low-dose aspirin has a role in stroke prevention, particularly among all the adult females.
Females account for the majority of American population of 64 years and older and for stroke deaths.
After a non-fatal stroke females suffer more significant disability than males.
Strokes killed twice as many females as breast cancer.
Risk factors that could predispose females to strokes include multiple pregnancies, preeclampsia, postpartum period, and migraine.
Antidopaminergic antiemetics are associated with be a threefold increased risk of stroke shortly after the initiation of treatment: domperidone, metopimazine, and metoclopramide.
Cause unknown in approximately 40% of patients after routine testing.
Higher incidence in blacks.
National Health and Nutrition Examination Surveys( NHANES) self-reported stroke prevalence among women 45 to 54 years of age with double that of similarly aged men.
There is an increasing stroke prevalence among women.
Obesity increases the risk.
Obese women with a BMI of 30 or greater have a 1.5 higher risk for total stroke, and a 1.7 fold higher risk for ischemic stroke.
Decreased risk associated with increased physical activity, so that a meta-analysis showed moderate intense physical activity is protective for total, ischemic, and hemorrhagic stroke (WENDEL VOS GC et al).
Tendency to cluster within families.
Risk associated with substantial genetic component.
In an analysis of four cohort studies of incident stroke common SNPs on chromosome 12p13 associated with total, ischemic and atherothrombotic stroke in white people (Ikram M).
Survivors are older, more likely to have chronic renal disease, hypertension, coronary artery disease, elevated hemoglobin A1c, and lowered hematocrit than in patients without stroke.
Most patients experience spontaneous physical improvement after a stroke, but recovery is generally incomplete.
A large prospective study of a combination healthy lifestyle activities including maintaining a normal BMI, regular ingestion of vegetables, participating in moderate or high level physical activity, never smoking, and having light to moderate alcohol consumption was associated with a substantially reduced risk of stroke (Zhang Y et al).
Alcohol consumption and stroke risk J-shaped in most studies, with the lowest risk among those consuming light to moderate amount of alcohol. In
In the above study at the five healthy lifestyle factors were associated with decreased risk of total, ischemic, and hemorrhagic stroke, and a stroke risk progressed steadily decreases as the number of healthy lifestyle factors increased.
One in four patients that have a stroke are under the age of 65 years.
Independently associated with impaired renal function.
Approximately 50,000 patients with valvular heart disease experience a first stroke each year in the U.S.
Ideal imaging study for patients with acute stroke should assess both cerebral ischemia, intracranial hemorrhage and discriminate cerebrovascular causes from other causes.
Brain CT is the most common imaging modality used to evaluate suspected stroke and is sensitive to acute intracranial bleeding but it is not sensitive to acute ischemic changes.
With brain MRI acute ischemic injury changes are detectable sooner than with CT.
With acute hemorrhagic strokes MRI and CT have similar diagnostic rates.
Lifetime cost of stroke exceeds $90,000 per patient for ischemic stroke and more than $225,000 for subarachnoid hemorrhage.
Fewer than 4% of patients are admitted to the hospital within 3 hours of stroke onset.
Severity of stroke-related disability can be reduced, if timely treatment is received.
Causes 12% of deaths complicating pregnancy.
Intravenous thrombolysis with tissue plasminogen activator (t-PA) is safe and improves outcome of ischemic strokes if initiated within 3 hours after onset of symptoms.Use of tissue plasminogen activator (t-PA) for ischemic stroke is uncommon with only 3-5% of such patients receiving the drug.
Intravenous thrombolytic therapy can reduce disability from ischemic strokes by one third.
European Cooperative Acute Stroke Study III (ECASS III) enrolled patients between 3 and 4.5 hours after the onset of symptoms and demonstrated evidence that thrombolytic therapy is safe and effective management.
In a retrospective analysis of the use of tPA for patients, 90 years old with acute ischemic stroke: by day 30 9% of patients had a favorable outcome, 9% had moderate disability, and most patients had severe disability or death (Mateen FJ).
Intravenous t-PA treatment in the age group of 90 or above does not improve the outcome of ischemic stroke.
Immediate goal of ischemic stroke is the restoration of cerebral perfusion via recanalization of the vascular occlusion.
Systemic thrombolysis results in complete recanalization in 20-66% of treated patients, but reocclusion occurs in more than 30% of such patients.
Studies have suggested annualized rate of stroke is 3% in women compared to 1.6% in men.
The majority are ischemic. Approximately 60% result from atherosclerosis in extracranial and larger intracranial vessels, 20% result from small-vessel lacunar disease, 15% are from cardiac emboli due to atrial fibrillation or myocardial infarction and 5% are the result of other unusual causes.
90% of patients with atrial fibrillation are receiving no warfarin or are taking sub therapeutic doses (Gladstone).
The rate of ischemic stroke among patients with atrial fibrillation is about 4.5% and warfarin usage lowers the rate to about 1.4%.
One of every six strokes occur in a patients with atrial fibrillation.
Approximately two-thirds of symptomatic strokes are caused by disease of large arteries more than 0.1 mm in diameter that run from the neck into the skull, the circle of Willis and surface of the brain.
Among 1487 patients outcome of stroke improved by evaluating swallowing, DVT prophylaxis and treating all episodes of hypoxia with oxygen supplemetation (Bravata DM).
Between 35-62% of stroke survivors develop some degree of cognitive impairment within 3 months of suffering the stroke.
Up to 85% of stroke survivors experience upper extremity impairment immediately after the event and between 55-75% of survivors experience continued functional problems up to 3-6 months later.
Half to two thirds of patients who survive regain independence and up to 80% of these patients retain or regain the ability to walk.
Half the deaths result from medical complications such as pneumonia and half attributable to neurologic complications.
Initial stroke with atrial fibrillation 71% die or have permanent neurological deficits.
New onset atrial fibrillation in severe sepsis associated with an increased risk of and hospital stroke and death, compared with patients with no atrial fibrillation and patients with pre-existing atrial fibrillation (Walkey AJ et al).
Increased stroke associated with infections, and is particularly demonstrated by the fact that patients with severe sepsis have a six fold increase risk of in-hospital stroke compared with hospitalized patients without severe sepsis.
Patients with chronic kidney disease and AF have a 3-fold higher risk for stroke.
Associated with atrial fibrillation have thrombus in the atrial appendage 90% of the time as demonstrated by transthoracic echocardiography.
A meta-analysis of trials comparing warfarin with placebo in nonvalvular AF in stroke prevention demonstrated a significant reduction in in stroke and all cause mortality in patients treated with warfarin (Hart RG et al).
Patients with AF at highest risk of stroke, those wth previous stroke or TIA with nonvalvular AF derive the greatest risk reduction of stroke with warfarin compared with aspirin or no antithrombotic treatment (Hart RG et al).
Current use (2012) of warfarin in nonvalvular AF is associated with a low rate of residual stroke or systemic embolism of an estimated rate of 1.66 per year (Agarwal S et al).
Overall mortality rate of 27%.
15% associated with arrhythmias.
After acute myocardial infarction patients have a very high hospital mortality of approximately 46%.
After CABG 1-6%.
Stroke in relation to coronary artery bypass graft ( CABG) may occur intraoperatively or postoperatively.
Stroke occurrence with coronary artery bypass graft is reduced when CABG is performed without cardiopulmonary bypass.
Among the 45,432 patients undergoing coronary artery bypass graft (CABG)_surgery 705 experienced a stroke, with 279 strokes occurring intraoperatively, and 58% postoperatively (Tarakji KG et al).
Relatively weak association with cholesterol level.
Intensive lipid lowering therapy with statins, ezetimbe, or proprotein convertase subtilisin/kexin inhibitors have been associated with lower risk of stroke in both primary and secondary prevention.
Statins reduce the risk of hemorrhagic stroke in both the lobe and non-lobe areas of the brain.
Stroke risks are reduced with long-term use of statins.
In elderly the frequency of strokes seems independent of plasma cholesterol.
Cholesterol lowering with statins proportionally reduces stroke risk.
Comparing people who have less than 3 fruit and vegetable servings per day with individuals with three to five servings per day there is a 11% reduction in the risk of stroke and in those with more than 5 servings per day there is a 26% reduction.
Cardiovascular risk factors include: hypertension, hyperlipidemia, diabetes mellitus, tobacco smoking, carotid disease, atrial fibrillation, and sickle cell anemia.
40% of patients experience depression during the first year following a stroke.
Depression associated with significant increased risk of stroke morbidity and mortality.
Depression may contribute to stroke through neuroendocrine, and immunological, and inflammatory effects.
Depression is associated with C-reactive protein, IL-1, and Il-6, and these inflammatory factors have been associated with increased risk of stroke.
Depression is associated with poor health behaviors such as smoking, physical inactivity, poor diet, poor medication compliance, and obesity, which may increase the risk of stroke.
Survivors of stroke with atrial fibrillation or 2.4 more times likely to develop dementia than those without atrial fibrillation.
Approximately 25% of patients with stroke and atrial fibrillation develop dementia during follow-up from three months to five years.
Diabetes increases risk of stroke 2-6 fold.
Diabetes is a primary risk factor for stroke.
Other conditions that can mimic a stroke include, seizures, neoplasms, subdural hematoma, hypoglycemia and other metabolic disorders and syncope.
Prevalence of obstructive sleep apnea syndrome among stroke patients is 60% compared to 4% in middle aged adults.
Data indicate obstructive sleep apnea in the pathogenesis of risk factors associated with stroke such as hypertension, coronary heart disease, diabetes, and atrial fibrillation which are believed to be mediated by adverse physiologic responses to recurrent periods of pharyngeal occlusion and oxyhemoglobin desaturation-re saturation.
The above responses result in the generation of free radicals, release of pro-inflammatory and prothrombotic mediators, endothelial dysfunction, increased sympathetic nervous system and increased blood pressure along with cerebrovascular alteration in auto regulation.
Obstructive sleep apnea increases the risk of stroke and prevalence in patients after a stroke.
Increasing the consumption of fruit and vegetables reduces the risk.
Troponin levels occur in approximately 17% of patients with adverse prognosis.
Patients with stroke should have a swallowing evaluation, DVT prophylaxis and oxygen treatment for all episodes of hypoxia to improve outcome (Bravata D et al).
Patients with severe stroke who require invasive mechanical ventilation are at high risk of death and poor functional outcome.
In stroke patients receiving mechanical ventilation early tracheostomy compared with standard approach does not significantly improve functional outcome at six months.
Prevalence of hypoxia in acute ischemic stroke patients is 13-15%.
20-30% of patients with stroke have swallowing abnormalities, and such abnormalities predict for chest infection and associated with a higher risk of death.
Correlates with vasculopathies involving the CNS and the onset of stroke: the worse the hyperglycemia the greater the risk of stroke downstream (Sui X et al).
In the presence of brain ischemia, elevated blood and brain glucose exacerbates ischemic neurologic injury, turning subclinical injury into apparent injury, and mild clinical injury into potentially debilitating or morbid illness (Wass CT et al).
Stroke prevention for men and women recommendations include: controlling blood pressure, avoiding or quitting smoking, maintaining a healthy weight, and exercise.
For stroke prevention for women with a history of hypertension low-dose aspirin, calcium supplement, or both should be considered to lower preeclampsia risk.
Women who have preeclampsia have twice the risk of stroke and 4 times the risk of hypertension later in life, compared with women who do not develop preeclampsia.
Intensive antiplatelet therapy does not reduce the incidence or severity of recurrent stroke or transient ischemic attack (TIA) in patients with recent cerebral ischemia, and significantly increases the risk of major bleeding, according to the results of a recent study.
Antiplatelet therapy with 3 agents has been suggested to potentially be more effective than recommended treatment for the prevention of recurrent ischemic events in patients with acute cerebral ischemia.
In an international, prospective, randomized, open-label, blinded-endpoint trial, researchers compared the safety and efficacy of antiplately therapy with aspirin, clopidogrel, and dipyridamole with guideline-based antiplatelet therapy.
The above trial involved 3096 participants, randomly assigned 1:1 to receive either guideline-based therapy (clopidogrel alone or combined aspirin and dipyridamole) or intensive therapy (combined aspirin 75 mg, clopidogrel 75 mg, and dipyridamole 200 mg twice daily).
Attempts to reduce stroke risk from the use of dual antiplatelet agents has been disappointing, showing no benefit but an increased risk of hemorrhage.
Overall, the incidence and severity of recurrent stroke or TIA was not different between the intensive and guideline-based treatment groups (6% vs 7%, respectively).
The intensive therapy was associated with more frequent and severe bleeding than guideline-based treatment.
In response to these findings, the trial was stopped early on the recommendation of the data monitoring committee.
Among patients with recent cerebral ischemia, intensive antiplatelet therapy did not reduce the incidence and severity of recurrent stroke or TIA, but did significantly increase the risk of major bleeding.
Triple antiplatelet therapy should not be used in routine clinical practice.
Mobile stroke units or ambulances with staff and computer tomographic scanner that may enable faster treatment with tissue plasminogen activator (t-PA) than standard management by emergency medical services.
In patients with acute vascular brain injury, preventive normothermia effectively can reduce fever burden, but does not improve functional outcomes (INTREPID study group).