 A focal infection of the paraspinal epidural space with accumulation of pus within the spinal canal between the vertebral column and the dura mater.
A focal infection of the paraspinal epidural space with accumulation of pus within the spinal canal between the vertebral column and the dura mater.
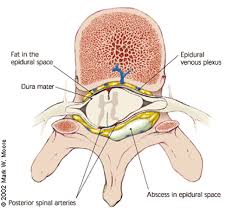
The infection in the epidural space which is located between the dura mater which surrounds the spinal cord or cauda equina and the osseus and ligamentous structures of the spine.
Rare process that is increasing in incidence because of aging population, increased use of spinal instrumentation, vascular access devices and intravenous drug abuse.
Osteophytes and intervertebral disc protrusions may reduce the size of the ventral epidural space, decreasing the potential volume before spinal epidural abscess has a neurological effect.
A potentially devastating infection, which eludes early diagnosis.
Local manifestations are described as a sequential four phase pattern of symptoms: phase 1, localized pain, phase 2, nerve root pain, phase 3, early neurologic changes of muscle weakness, sphincter impairment, and sensory deficit, and phase 4, paralysis.
Stage three neurologic symptoms of present at diagnosis in 20 to 47% of patients.
Motor or sensory deficits are reported more commonly than bowel bladder symptoms.
Stage four symptoms of paralysis or a complete neurologic deficit are present in approximately 3 to 9% of patients.
1/3 patients have symptoms for more than two weeks before diagnosis.
Neurologic symptoms are typically present for less than one week before diagnosis.
The potential for neurological impairment from a spinal epidural abscess within the cervical and thoracic spine is greater than the lumbosacral spine given the presence of the spinal cord, rather than cauda equina, at those levels, decreased canal volume, and tenuous blood supply in the cervicomedullary and mid thoracic regions.
Direct compression of the spinal cord or cauda equina is probably the predominant cause of neurological impairment, although local inflammation leading to thrombosis of vasospasm of the arterial supply of the spinal cord or compression by the abscess on the arterial supply may also occur.
Symptoms of bacterial meningitis may accompany spinal epidural abscess.
Systemic symptoms of infection include fever and sepsis in 25 to 62% of patients.
Contiguous spinal epidural abscesses are associated with infection of a nearby vertebral or extra vertebral structure.
Infected vertebral structures may include into vertebral discs, vertebral bodies, or facet joints, or a combination of these.
Contiguous extravertebral sites include paraspinal muscles, retropharyngeal space, posterior mediastinum, posterior pleural space, psoas muscles, and decubitus ulcerations.
Contiguous infection is the most common cause of spinal epidural abscess.
Surgical side infection associated spinal epidural abscesses occur after spinal surgery or procedures involving the spine.
Isolated, spontaneous, spinal epidural abscess can originate from direct hematogenous seeding of the epidural lymphatic vessels without evidence of continuous infection.
Infections at other sites, including endocarditis are not uncommon.
Incidence rates 2 -5.1 per 100,000 hospital admissions.
Increasing incidence related to rising number of patients with predisposing conditions, improved diagnostics and changing hospital referral patterns.
Predisposing processes include: diabetes, alcoholism, presence of HIV, spinal degenerative joint disease, spinal trauma, previous spinal surgery, spinal drug injections, placement of stimulators or spinal catheters, presence of infections of skin soft tissues, osteomyelitis, cancer, renal or hepatic insufficiency, urinary tract infection, aging, sepsis, presence of an indwelling vascular, intravenous drug abuse, epidural analgesia and prior nerve block.
The most common comorbidities for patients with spinal epidural abscess include: previous focus of infection, diabetes, intravenous drug abuse, and renal disease.
Most patients (84%) have identifiable risk factors, most commonly diabetes, intravenous drug use, immunosuppression, chronic renal failure, or recent spinal procedures.
Rising prevalence of predisposing factors, especially substance abuse, explain increasing incidence rate of these infections.
The thoracic spine is most frequently affected, often involving multiple contiguous or noncontiguous levels.
Abscesses occur within the epidural space between the spinal dura and vertebral periosteum and can result in spinal nerve compression and vascular damage.
Patients with spinal epidural abscess most commonly presented with axial pain which is present in over 2/3 of patients.
Classic triad of fever, actual pain, and neurologic deficit is seen in only 8% of patients.
patients typically present with localized back or neck, pain, or both, accompanied by fever or neurologic symptoms.
The classic triad of fever, back pain, and neurologic deficit occurs in less than 8% of patients.
Back pain is the most common presenting symptom, while fever is absent in 50% and neurologic abnormalities occur in approximately half of cases.
This nonspecific presentation contributes to misdiagnosis in up to 90% of patients on their first emergency department visit.
Concurrent illness can result in immune compromise in as many as 60% of patients with spinal epidural abscess.
Diabetes is often the most common predisposing factor.
Intravenous drug use is an emerging risk factor.
Iatrogenic factors such as spinal surgery, spinal procedures and central intravenous lines may be important contributors.
In about one third of cases bacteria spreads to the epidural space contiguously, in half of the cases hematogenously and in the rest the source of the infection is not identified.
In cases of unknown source, it is suspected that hematogenous seeding occurs during a transient bacteremic episode.
Continuous spread may come from vertebral osteomyelitis, or psoas abscess.
Direct spread by inoculation from recent surgery or spinal procedure.
Most predisposing conditions result from Staphylococcus aureus skin flora in about two thirds of cases.
The lumbar and lumbosacral levels are the most frequent sites of spinal epidural abscess, accounting for 50% of all infections.
About 30 to 40% of spinal epidural abscesses occur in the thoracic spine, with the remaining 10 to 20% involving the cervical spine.
Most infections span 2-3 vertebral levels, and skip lesions are commonly observed.
In most studies, ventral spinal epidural abscesses are more common than dorsal spine epidural abscesses.
The preponderance of ventral spinal epidural abscesses reflects the frequency of concomitant vertebral osteomyelitis, spondylodiscitis and psoas muscle abscesses, collectively found in more than 50% of cases.
Common bacterial pathogens include: Staphylococcus aureus, coagulate negative staphylococcus, E. coli, Pseudomonas aeruginosa, and fungal agents like Canida.
66% of patients have leukocytosis and an elevated ESR and C reactive protein which are noted in nearly all patients.
Associated with positive blood cultures in 63-70% of cases, and the positive culture corresponds to the offending organism nearly 100% of the time, which is most often Staphylococcus aureus.
Typically occurs in 6th-7th decades.
Consequences of late diagnosis includes paraplegia, quadriplegia and death.
More frequent in males.
Most common complaint is pain, usually without constitutional symptoms.
Diagnosis usually by CT guided bone biopsy and culture.
MRI with gadolinium or CT with myelography are the two major imaging will galleries available to evaluate epidural abscesses.
Gadolinium-enhanced MRI of the entire spine is the diagnostic modality of choice, and blood cultures should be obtained.
Imaging modalities should be obtained of the entire spinal axis, that is the cervical, thoracic, and lumbar sacral spines due to the possibility of infectious foci at multiple spinal locations.
Both of the above imaging modalities produce similar diagnostic sensitivity of 90% and above.
Management is based on the patient’s medical history, the infectious organisms, the location and size of the abscess, and most importantly the neurologic examination.
Emergency referred to spine and infectious disease specialists are warranted.
Decompression and debridement surgery followed by long-term antibiotics is the treatment of choice and significantly improves the outcome in patients with neurological compromise.
An accurate microbiological diagnosis is essential and can be made with blood cultures, tissue and fluid cultures obtained by image guided needle aspiration or biopsy, or at the time of surgery.
Treatment typically involves emergent surgical decompression and debridement followed by prolonged antibiotic therapy, though carefully selected patients without neurologic deficits may be candidates for medical management alone.
MRI with contrast enhancementis the diagnostic imaging modality of choice as it is less invasive and provides improved soft tissue detail.
Management requires drainage and antimicrobial therapy.
Antimicrobial therapy alone may be curative and carefully selected patients.