 Implies compression of the thecal sac by tumor in the epidural space at the level of the spinal cord or cauda equina.
Implies compression of the thecal sac by tumor in the epidural space at the level of the spinal cord or cauda equina.
Divided into intradural (intramedullary and leptomeningeal) and extradural lesions.
The natural history leads to pain, paralysis, sensory loss, and sphincter dysfunction.
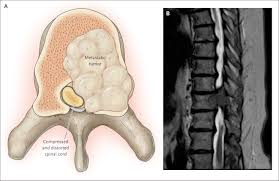
Most cases caused by direct extension of a metastasis in the vertebral body to the spinal cord.
Estimated 12,700 cases per year in United States with breast, prostate, and lung cancer each accounting for 15 to 20% of cases.
75% of cases have an associated soft tissue epidural metastases.
25% of patients have bone collapse with bone fragments adding to the compression.
Upper motor neuron syndrome typically present with spinal cord compression but its absence does not exclude severe disease.
2.54% of patients that die from progressive cancer will have at least one episode of spinal cord compression in their last 5 years of life.
Epidural spinal cord compression affects the thoracic spine in approximately two thirds of patients, the lumbar spine in about one fifth of patients and the cervical spine in the remainder of the patients.
Location of the lesion is proportional to the volume or mass of bone present in each region.
Breast and lung cancer have a predilection for the thoracic spine, whereas colon and pelvic neoplasms commonly affect the lumbar spine.
Incidence varies by primary cancer site, from 7.9% in myeloma, to 0.2% in patients with pancreatic cancer (Loblaw DA et al).
10-38% of patients have compression at multiple sites.
New cord lesions with compression arise in a different site in approximately 10% of individuals with a median occurrence of 4.5 months after the initial manifestation of spinal cord disease.
Approximately 75-100% of patients who are ambulatory at the time of treatment remain so, whereas only 14-35% of nonambulatory patients and 5% of paraplegic patients regain useful function after undergoing surgery or radiotherapy.
Malignant extradural prognosis is poor with a median survival of 2.9 months after diagnosis (Loblaw DA et al).
Tumor histology relates to prognosis with overall survival worst for non-small cell lung cancer of 1.5 months, and the best for myeloma with a median overall survival of 6.7 months.
Prognostic factors include: tumor histology, the presence of visceral metastases, other bone metastases, ambulatory status before treatment, time interval between tumor diagnosis and the development of spinal cord compression, and the time to developing motor deficits (Rades D et al).
Rades prognostic score for malignant epidural spinal cord compression
Prognostic factor Score
Type of tumor
Myeloma/lymphoma 9
Breast ca 8
There is a three fold difference in overall survival if a patient is ambulatory after treatment-10 months vs. 3 months (Maranzano e et al).
MRI is an effective noninvasive technique for diagnosis.
Prostate, breast and lung cancer each account for 15-20% of cases, non-Hodgkin�s lymphoma, multiple myeloma, and renal cell cancer account for 5-10% each, and colorectal cancer, cancer of unknown primary and sarcoma account for most of the remaining cases.
Develops in approximately 10% of patients with prostate cancer at some point in the course of their disease.
For metastatic spinal cord compression from prostate cancer, steroids and surgery followed by radiation would be standard therapy.
In patients with metastatic spinal cord compression who are not surgical candidates 30 Gy in 10 fractions is standard therapy.
The prognosis for patients with metastatic spinal cord disease is grouped based on 5 factors: Ambulatory or not status, performance status, other bone metastases, visceral metastasis, and interval from cancer diagnosis radiotherapy.
Is the initial manifestation of cancer in 20% of such patients, with lung cancer accounting for 30% of these patients.
Cumulative incidence for patients 40-60 years of age is 7.3% for patients with breast cancer, 15.3% for patients with myeloma and 16.9% for patients with prostate cancer.
The mainstays of treatment are prompted initiation of corticosteroids to reduce edema, surgical intervention and radiotherapy.
In patients with limited metastases, good performance status or early onset of paraplegia, (within 48 hours), and who are surgical candidates, surgery in addition to radiation improves the ability to walk.
In patients who are ambulatory prior to treatment 94% will be able to walk with the combination of surgery and radiation, versus 74% for those treated with radiation alone, and for patients who are nonambulatory at presentation the numbers are 62% versus 19%, respectively.