
 A state of cardiovascular dysfunction associated with infection and unexplained by other causes.
A state of cardiovascular dysfunction associated with infection and unexplained by other causes.
Sepsis and septic shock affect over 30 million people globally and results in the mortality rate of approximately 25%-50%.
A leading cause of death worldwide.
An estimated 48.9 million cases of sepsis and 11 million related deaths occur annually, worldwide.
In the US more than one third of in-hospital deaths are attributed to sepsis, which makes it the most common cause of in-hospital death, and the most expensive cause of hospitalization.
A subset of sepsis in which circulatory, cellular, and metabolic abnormalities are associated with the greater risk of mortality then sepsis alone.
New clinical criteria representing the definition of septic shock includes the need for vasopressor therapy to maintain a mean arterial pressure of 65 mmHg or greater in the presence of a serum lactate level of greater than 2 millimoles /L persisting after fluid resuscitation.
Refers to life-threatening circulatory failure with inadequate tissue perfusion.
The vasculature is a key site of injury with sepsis, with endothelial cells expressing cytokines, chemokines and damage signals as a response to pathogens and tissue injury.
During sepsis, blood vessels shed their protective barrier that insulates them from circulating blood and platelets with formation of leukocyte and platelet adhesion.
Activation of the complement system during sepsis insights tissue damage and microvascular thrombosis.
With sepsis regulation of the endothelial permeability is often lost, and this vascular dysregulation is manifested as hypotension, third spacing of fluid, and in rare cases disseminated intravascular coagulation.
Typical presentation is hypotension with systolic blood pressure 90 mg of mercury or less or mean arterial blood pressure of 65 mmHg or less accompanied by signs of hypoperfusion.
The most common cause of non-cardiogenic shock.
Occurs in more than 230,000 patients each year with more than 40,000 deaths annually.
The primary risk factors for septic shock are infection and it is the fifth leading cause of years of productive life lost due to premature mortality.
Early resuscitation is a key factor to limit progression to multiple organ dysfunction and death in patients with septic shock.
Shock is characterized by increased serum lactate levels and signs of tissue hypoperfusion including abnormal peripheral perfusion.
More than 750,000 cases of severe sepsis and septic shock annually in US.
Using the Surviving Sepsis Campaign guidelines has showed survival benefits in a number of randomized studies.
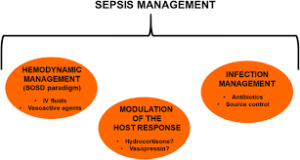
Management of sepsis focuses on infection control, restoration of perfusion and organ support.
Trials comparing liberal versus restrictive fluid administration of high versus low mean arterial pressure targets have failed to improve patient centered outcomes.
Septic shock resuscitation relies on the assumption that hemodynamic optimization will improve tissue, perfusion and revert cell metabolic arrangements.
Capillary refill time may identify tissue hypoperfusion and could reflect the progress of resuscitation.
Targeted resuscitation is associated with faster, recovery of organ dysfunction, less fluid administration, and a higher likelihood of survival compared with lactate targeted resuscitation.
Pathogenic mechanism, such as hypovolemia, vasoplegia, and cardiac dysfunction are involved in overlap in septic shock.
The ANDROMEDA -2 shock trial a personnel personalized hemodynamic resuscitation strategy involving capillary fill strategy and its normalization improves patient centered outcomes in early septic shock.
Treatment of infection includes antimicrobial therapy for all suspected bacterial/fungal infections and for many parasitic and viral infections.
The initial antimicrobial therapy is often an empirical.
Initial antimicrobial regimens are considered based on the site of infection, likely pathogens, local epidemiologic factors, risk factors, consideration of possible susceptibilities, predisposition to specific infections, social history, exposure to atypical pathogens, etc.
Prompt initiation of antimicrobial therapy is warranted as mortality increases with delays in treatment administration
However, in randomized trial conducted in 31 academic centers Protocolized Care for Early Septic Shock (ProCESS), protocol based resuscitation with EGDT and protocol based standard therapy was not associated with a survival benefit.
In a randomized trial at 51 centers in Australia, EGDT therapy in critically ill patients presenting to the emergency department with early septic shock did not produce all cause mortality at 90 days (ANZICS Clinical Trials Group).
The disruption of the hypothalamic-pituitary-adrenal axis is considered a key process in the progression from infection to septic shock.
Hydrocortisone does not improve survival or reverse shock, although in patients in whom shock was reversed it hastened the reversal.
In a randomized controlled study of hydrocortisone 200 mg/d in eight patients with septic shock a lower mortality in those treated for seven days, vs. three days at 24% vs. 32%), respectively(Huh JW).
Trials of high-dose corticosteroids, usually given as a single by Alyssa, was not associated with survival benefits (Cronin L).
Randomized studies using 300 mg per day of hydrocortisone or equivalent doses of other agents for greater then five days indicated some improvement in survival in a septic shock patients (Minneci PC, Annane D).
A multi-center study with hydrocortisone therapy in septic shock patients indicated no significant benefit to risk ratio (Sprung CL).
In a review of 17 randomized trials and three partial randomized trials using corticosteroids vs. placebo or supportive treatment in adult patients or severe sepsis revealed: Overall, corticosteroids did not affect 28 day all-cause mortality, and to prolonged low dose corticosteroid treatment had a favorable effect on all-cause mortality (Annane D).
In the above study steroids in this setting did not provide robust improvement and the authors suggested treatment with hydrocortisone or equivalent drugs at a daily dose of 200 to 300 mg given a full dose for at least 100 hours and only in adults with vasopressor dependent shock (Annane D).
Evidence does not support the use of short course of high dose corticosteroids in severe sepsis or septic shock.
Is the most severe manifestation of sepsis.
Refers to sepsis induced hypotension that persists despite adequate fluid resuscitation.
May be present with hypotension with systolic blood pressure less than 90 mm Hg or in the presence of a 40 mm Hg drop from baseline with resulting organ dysfunction from perfusion impairment and lactic acidosis, impaired mentation and oliguria.
Intravenous crystalloid fluid is the first line treatment to correct intravascular, volume depletion and restore preload.
Guideline suggest 30 mL per kilogram of body weight as a reasonable initial fluid volume for most adult patients, and the fluid should be delivered in serial bonuses with close monitoring of the clinical response.
Underresuscitation and overresuscitation are associated with harm, and show a U-shaped relationship between fluid volume and outcomes.
Occurs in 2-20% of hospitalized patients.
Most common cause of death in ICU’s
Resuscitation efforts include use of intravenous fluids and catecholamines norepinephrine, epinephrine, dopamine, and dobutamine.
Intravenous fluids are administered to improve circulation in these patients and guidelines suggest an initial fixed volume of 30 mL per kilogram of body weight, although the level of certainty for this evidence is low.
The use of higher volumes of intravenous fluid is associated with harm in observational studies and in randomized controls trials, of patients with sepsis and septic shock.
Among adult patients with septic shock in the ICU, intravenous fluid restriction did not result in few or deaths at 90 days and standard intravenous fluid therapy (CLASSIC trial group).
Lactate clearance is a calculated change from 2 specimens of blood drawn at different times is a method of assessing tissue oxygen delivery.
Lactate clearance basis presumes shock causing inadequate oxygen deklivery causing mitochondrial hypoxia.
Mitchondrial hypoxia causes oxidatice phosphorylation failure and anaerobic glycolysis pursues with an increase in lactate production.
Anaerobic glycolysis increases cellular lactate which then enters the blood.
Blood lactic acid levels varies with oxygen deficit in tissues.
Abilitry of the body to reduce lactate levels in the blood reflects restoration of oxygen delivery.
Lactate clearance of 10% or more predicts survival from septic shock.
Alpha-adrenergic effects increased vascular tone but may decrease cardiac output and regional blood flow, especially in cutaneous, splanchnic, and renal beds.
Beta-adrenergic effects help to maintain blood flow through inotropic and chronotropic effects and to increase splanchnic perfusion.
Beta-adrenergic effects can have unwanted consequences including increasing cellular metabolism and immunosuppressive effects.
Dopamine stimulates dopaminergic receptors and proportionally has a greater increase in splanchnic and renal perfusion and may facilitate resolution of lung edema(Bertollo AM).
In a randomized multicenter controlled study in patients with shock that received dopamine or norepinephrine as first line vasopressor therapy to restore and maintain blood pressure:there was no difference in the death rate between the two gents, but the use of dopamine was associated with a greater number of adverse events, especially arrhythmias (De Backer D).
In the above study a subgroup analysis indicated that at 28 days the dopamine group death rate was higher than the norepinephrine group with cardiogenic shock but nor for patients with septic shock(De Backer D).
Dopaminergic stimulation at 28 days can alter among patients the hypothalamus-pituitary function with a decrease in prolactin levels and growth hormone levels.
Dopamine and norepinephrine have different effects on the kidney, splanchnic vessels, and the pituitary axis.
Either dopamine or norepinephrine can be used as the first agent for vasopressor effect in patients with shock.
Some studies show that the administration of dopamine may be associated with higher death rates than those associated with the administration of norepinephrine with septic shock (Martin C, Boulain T).
Following sepsis patients have elevated circulating pro-inflammatory cytokines for weeks after resolution of the infection.
Use of catecholamines can reestablish blood pressure to maintain organ perfusion, but have adverse effects including increased mortality rates.
In healthy volunteers challenged with endotoxin low dose corticosteroids prevent release of pro-inflammatory cytokines, and activation of endothelial cells and neutrophils(de Kruif MD).
In healthy volunteers challenged with low dose corticosteroids acute phase responses are inhibited and alteration of coagulation-fibrinolysis balance is not altered (de Kruif MD).
Low dose hydrocortisone has no significant effect on rate of death in patients with septic shock at 28 days (Sprung).
Use of hydrocortisone may increase incidence of superinfections and new septic episodes.
IV hydrocortisone 200 mg/day is suggestive for patients who are hemodynamically unstable despite fluids and vasopressors.
Recommendations for patients with hypoperfusion is that they should receive at least 30 mL per kilogram of IV crystalloid within three hours.
For patients who require vasopressors, the initial target mean arterial pressure should be 65 mmHg.
IV antibiotics should be started within one hour of sepsis recognition and should include combination therapy of at least two classes of antibiotics‘s to cover a known or suspected pathogen for patients with septic shock.
Norepinephrine is the first choice for patients who need vasopressors and vasopressin or epinephrine can be added: Dobutamine is recommended for patients who remain stable.
Transfusion should be reserved for patients with hemoglobin concentration less than 7 g/dL, except in special circumstances such as hemorrhage or myocardial ischemia.
A three day course of corticosteroids can reduce symptoms of systemic inflammation and reduces the amplification of the systemic inflammatory response space (Keh D).
Sodium bicarbonate should not be used for most patients pH greater than 7.15.
In patients with septic shock who underwent transfusion and hemoglobin threshold of 7 g/dL, as compared with those who underwent transfusion at hemoglobin threshold of 9 g/dL received fewer transfusions and had similar mortality at 90 days, use of life support, number of days alive and out of the hospital, and the numbers of patients with ischemic events and severe adverse reactions to blood were similar in the two groups (Holst LB et al).
In patients with septic shock treatment with intravenous vitamin C, hydrocortisone, and thiamine compared with intravenous hydrocortisone alone did not show significant improvement in the duration of time alive and free of vasopressor administration over seven days (Vitamin trial investigators).