 Refers to the retroperitoneal space which is bordered anteriorly by the posterior parietal peritoneum, posteriorly by the transversalis fascia, and superiorly by the diaphragm.
Refers to the retroperitoneal space which is bordered anteriorly by the posterior parietal peritoneum, posteriorly by the transversalis fascia, and superiorly by the diaphragm.
The anatomical space in the abdominal cavity behind the peritoneum.
The retropritoneum has no specific anatomical structures.
The retroperitoneal space lies directly posterior to the peritoneal cavity.
An organizational schema dividing the retroperitoneal space into three different zones.
Also, the retroperitoneum contains vital musculoskeletal structures such as the psoas muscles, vertebra, quadratus lumborum, and iliacus muscles.
It houses connections to the diaphragm and bony pelvis.
Organs are retroperitoneal if they have peritoneum on their anterior side only.
Structures not suspended by mesentery in the abdominal cavity and that lie between the parietal peritoneum and abdominal wall are retroperitoneal.
An organizational schema divides the retroperitoneal space into three different zones.
The central-medial zone (Zone I) falls between the two psoas muscles and contains midline structures such as the abdominal aorta, inferior vena cava, pancreas, and duodenum.
The perirenal zone (Zone II) begins lateral to the psoas muscles on either side and contains the kidneys, ureters, and portions of the colon.
The pelvic zone (Zone III) includes the bladder as well as a multitude of vascular structures, including a robust network for presacral veins.
The retroperitoneum contains vital musculoskeletal structures such as the psoas muscles, vertebra, quadratus lumborum, and iliacus muscles.
It houses connections to the diaphragm and bony pelvis.
Primarily retroperitoneal organs include: adrenal glands, kidneys, ureter, bladder, aorta, IVC, thoracic esophagus, part of the rectum.
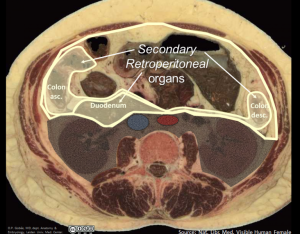
Organs once suspended within the abdominal cavity by mesentery but migrated posterior to the peritoneum during the course of embryogenesis to become retroperitoneal are secondarily retroperitoneal organs and include: head, neck and body of the pancreas, the duodenum, except for the proximal first segment, which is intraperitoneal, ascending and descending portions of the colon
It extends to the level of pelvic brim inferiorly.
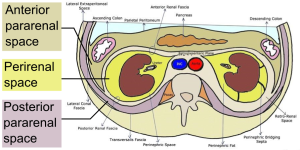
The anterior and posterior layers of renal fascia, also known as Gerota fascia, subdivide the retroperitoneal space on either side of the spine into 3 compartments.
The anterior pararenal space is bordered anteriorly by the posterior parietal peritoneum, posteriorly by the anterior layer of renal fascia, and laterally by the lateral conal fascia.
The retroperitoneal space is bordered anteriorly by the posterior parietal peritoneum, posteriorly by the transversalis fascia, and superiorly by the diaphragm.
The anterior and posterior layers of renal fascia, known as Gerota fascia, can subdivide the retroperitoneal space on either side of the spine into 3 compartments.
The posterior space contains the pararenal fat.
The intermediate space contains the kidney, the adrenal gland, and the perirenal fat.
The anterior space is more extensive:
The anterior pararenal space is bordered anteriorly by the posterior parietal peritoneum, posteriorly by the anterior layer of renal fascia, and laterally by the lateral conal fascia.
The anterior pararenal space contains the extraperitoneal portions of the ascending and descending colon, the duodenum, and the pancreas.
The anterior pararenal space is continuous across the midline.
Medially, the anterior layer of renal fascia blends with the connective tissue around the aorta and the inferior vena cava.
The posterior layer fuses with the psoas fascia.
Laterally, both layers merge to form lateral conal fascia.
The anterior pararenal space contains the extraperitoneal portions of the ascending and descending colon, the duodenum, and the pancreas.
The anterior pararenal space is continuous across the midline.
RP masses can be found within retroperitoneal organs or externally, and its location directs how the patient clinically presents.
RP masses located near the kidney and ureters can cause a patient to present with decreased urinary output, flank pain, and renal failure.
A RP mass near the duodenum may be associated with gastric outlet obstruction with nausea, vomiting, and early satiety.
CT scans or MRI are the best imaging techniques to evaluate the retropritoneum.
Of the primary RP masses approximately 70% to 80% are malignant.
Malignant retroperitoneal masses represent less than 0.5% of all malignancies.
RP masses are typically biopsied in order to identify the tissue Type.
RP mass lesions include: sarcomas, schwannomas, pheochromocytomas, and germ cell tumors, lipomas, fibromas, and gastrointestinal stromal tumors.
The treatment of RP masses, vary based upon the tissue diagnosis and staging, but can include surgery, radiation, and chemotherapy.