Radiation pneumonitis refers to the acute manifestation of radiation-induced lung disease.
It relatively common following radiation therapy for chest wall or intrathoracic malignancies.
RN typically occurs between 4-12 weeks following completion of radiotherapy.
Manifests from 2 weeks to 6 months after completion of radiation and is often reversible with corticosteroids.
Radiation toxicity is clinically significant in 10 to 30% of patients treated with thoracic radiation therapy manifesting with dyspnea, nonproductive, cough, pleuritic, chest pain, fever, and rarely, acute respiratory distress syndrome.
Radiation pneumonitis reduces quality of life with fatal toxicity occurring in 2% of patients with cancer.
RN may be seen as early as one week, in patients receiving a high total dose of radiation and/or also having received chemotherapy.
Symptoms of RN include:
cough
dyspnea
low-grade fever
chest discomfort
pleuritic pain
The lungs are the most sensitive organ when irradiating the chest.
Radiation pneumonitis changes:
loss of type I pneumocytes
increased capillary permeability
interstitial and alveolar edema
ingress of inflammatory cells into the alveolar spaces
Changes may be seen in the contraleteral non-irradiated lung due to suspected immune-mediated lymphocytic alveolitis.
Chest x-ray changes are non-specific are are usually confined to the irradiation port.
Findings include primarily airspace opacities.
Pleural effusions or atelectasis May occur.
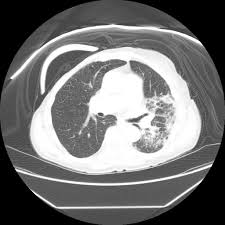
CT thorax can better delineate parenchymal lung changes than chest X-rays.
CT thorax demonstrating changes localized to the irradiated field, makes the diagnosis easier.
With stereotactic ablative radiotherapy the shape of the irradiated field does not conform to the traditional conventional radiotherapy portals.
Areas of ground-glass opacity may be evident on CT despite a normal chest x-ray
CT thorax most common findings are ground-glass opacities and/or airspace consolidation.
CT thoracic opacity findings:
halo sign: lung consolidation surrounded by ground-glass opacities
reversed halo sign: ground-glass opacities surrounded by a crescentic or circumferential area of consolidation
nodule-like pattern
septal thickening may occur later with the alveolar opacities producing a crazy paving pattern
ipsilateral pleural effusion
atelectasis
pulmonary necrosis: rare
FDG-PET performed soon after completion of radiotherapy often demonstrates increased metabolic activity in both lungs.
Only a minority of patient go on to develop clinically or CT evident pneumonitis.
FDG avidity in the radiation treated area is usually present in late phases of radiation pneumonitis, the 3 to 9 month period after treatment completion.
This avidity is due to the presence of residual inflammation and, therefore, PET-CT is of equivocal clinical value in this period.
Steroids reduce the severity of acute radiation pneumonitis.
Lung changes may be mild and spontaneously resolve or progress adult respiratory distress syndrome with a high rate of mortality.
Chronically radiation fibrosis may occur in some.
Where a clear demarcation that conforms to the irradiation port there is little difficulty in making the diagnosis.
Diagnosis is forthcoming when a history of chest radiotherapy is known, and c knowledge of the time course of the changes concerning radiotherapy, total dose administered, coadministration of chemotherapy, and shape of the portal field.