 Refers to a malformation of the head marked by an oblique slant to the main axis of the skull.
Refers to a malformation of the head marked by an oblique slant to the main axis of the skull.
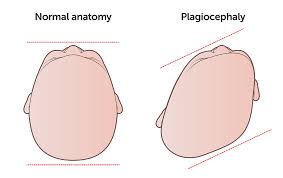
Plagiocephaly, also known as flat head syndrome, is a condition characterized by an asymmetrical distortion of the skull.
There is flattening of one side of the skull.
It is characterized by a flat spot on the back or one side of the head caused by remaining in a supine position for prolonged periods.
There is often some facial asymmetry.
Plagiocephaly divides into two groups: synostotic, with one or more fused cranial sutures, and non-synostotic deformational.
Brachycephaly refers to a very wide head shape with a flattening across the whole back of the head.
Slight plagiocephaly is routinely seen at birth and may be the result of a restrictive intrauterine environment.
It presents as a “diamond” shaped head when seen from above.
The incidence of plagiocephaly has increased since the advent of anti-sudden infant death syndrome recommendations for parents to keep their babies on their backs.
The rates of plagiocephaly are higher for twins and multiple births, premature babies, babies who were positioned in the breech position or back-to-back, as well as for babies born after a prolonged labor.
Plagiocephaly is seen in:
Arthrogryposis, cleft palate, craniosynostosis, and impaired intellectual development
Autism, susceptibility, X-linked
Blepharophimosis-impaired intellectual development syndrome
Cardiac anomalies – developmental delay – facial dysmorphism syndrome
CHIME syndrome
Coffin-Siris syndrome 1 and 6
Congenital nonprogressive myopathy with Moebius and Robin sequences
Cornelia de Lange syndrome
Cranioectodermal dysplasia
Craniosynostosis (nonsyndromic)
Developmental and epileptic encephalopathy
Developmental delay with variable intellectual impairment and behavioral abnormalities
Dihydropyrimidinase deficiency
Early-onset progressive diffuse brain atrophy-microcephaly-muscle weakness-optic atrophy syndrome
Faciocardiorenal syndrome
FG syndrome
Galloway-Mowat syndrome
Gaze palsy, familial horizontal, with progressive scoliosis
Hyperphosphatasia with intellectual disability syndrome
Hypotonia, infantile, with psychomotor retardation and characteristic facies
Intellectual developmental disorder, autosomal dominant
Intellectual disability, autosomal dominant Joubert syndrome
Kleefstra syndrome
Langer-Giedion syndrome
Microphthalmia with brain and digit anomalies
Mitochondrial DNA depletion syndrome
Muenke syndrome
Noonan syndrome
Osteogenesis imperfecta, type
Ritscher-Schinzel syndrome
Plagiocephaly with oxycephaly in Saethre-Chotzen syndrome
Saethre-Chotzen syndrome
Spastic paraplegia, intellectual disability, nystagmus, and obesity
Syndromic X-linked intellectual disability Najm type
It is also common for an infant with positional plagiocephaly to have misaligned ears,where the ear on the affected side may be pulled forward and down and be larger or protrude more than the unaffected ear.
Prevention methods: carrying the infant and giving the infant time to play on their stomach,which may prevent the baby from progressing into moderate or severe plagiocephaly.
Letting babies crawl may also prove to be crucial in preventing plagiocephaly by strengthenig babies’ spine and neck muscles.
Crawling also boosts gross and fine motor skills, balance, hand-eye-coordination and overall strength.
There are specialized mattresses available to prevent plagiocephaly, by reduces pressure on the baby’s head.
The condition may improve to some extent as the baby grows.
Home treatment or physical therapy treatment can improve the shape of a baby’s head.
Early interventions reduce the severity of the degree of the plagiocephaly.
Diagnosis is most commonly determined through clinical examination.
The Plagiocephaly Severity Scale can help practitioners evaluate the condition in a standardized way.
Treatment is typically based on the age of the child when the diagnosis is made in conjunction with the severity of the diagnosis.
If a diagnosis of mild to moderate plagiocephaly occurs before four months of age, repositioning therapy may be helpful.
If severe, a cranial molding orthosis (helmet) is prescribed between five and six months of age.
Initially, treatment usually takes the form of reducing the pressure on the affected area through repositioning of the baby onto their abdomen for extended periods of time throughout the day.
Treatment may include repositioning the child’s head throughout the day so that the rounded side of the head is placed against the mattress, repositioning cribs and other areas that infants spend time in so that they will have to look in a different direction to see their parents or others in the room, repositioning mobiles and other toys for similar reasons, and avoiding extended time sleeping in car seats, bouncy seats, or other supine seating which is thought to exacerbate the problem.
High quality evidence is lacking for cranial remolding orthosis for the positional condition and use for this purpose is controversial.
If conservative treatment is unsuccessful, helmets may help to correct abnormal head shapes.
These helmets are used to treat deformational plagiocephaly, brachycephaly, scaphocephaly and other head shape deformities in infants 3–18 months of age by gently allowing the head shape to grow back into a normal shape.
Some babies with plagiocephaly may comprise a high-risk group for developmental difficulties.
Plagiocephaly is associated with motor and language developmental delays.
Developmental delay is more commonplace among babies with plagiocephaly, it cannot be inferred that plagiocephaly is the cause of the delay.
Presently the term has been applied to any condition characterized by a persistent flatten spot on the back or side of the head, also known as flat head syndrome.
Untreated children with plagiocephaly may experience other medical issues later in life.
The increase in the number of children with flatten heads attributed to the movement of having babies sleep on their backs.
The process can be much worse on one side if a child preferentially sleeps with that side down.
Deformational brachycephaly is a flattening across the back of the head.
Plagiocephaly and brachycephaly can occur together.
Common presentation at birth and may be the result of a restrictive intrauterine environment.
Often caused by inability of the infant to turn their head in one direction due to neck pain from torticollis.
Treatments range from a simple repositioning of babies below the age of 5 months to use of helmets in children under the age of 18 months.
No evidence to suggest that plagiocephaly is harmful to neurological development.
The condition will sometimes improve with time, but in many cases, ttreatment usually takes the form of reducing the pressure on the affected area through repositioning of the baby onto his or her abdomen.
Treatments include repositioning the child’s head throughout the day.
Helmets are used to treat deformational plagiocephaly, brachycephaly, scaphocephaly and other head shape deformities in infants 3–18 months of age.
A helmet, ref2242ed to as cranial remolding orthosis provides a pathway for more symmetrical skull growth.
Treatment generally takes 3–4 months,.