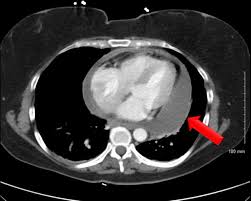
 Accumulation of fluid within the pericardial sac.
Accumulation of fluid within the pericardial sac.
Most frequent caused by damage to the lining of the cavity and increased permeability of the capillaries.
Acute pericarditis associated with pericardial venous and lymphatic drainage interference that predisposes to the development of effusion.But
If fluid accumulates rapidly or reaches a large volume it may cause the vena cava and the atria to compress and lead to cardiac tamponade.
30% cases due to metastatic cancer, 22% to chronic renal failure, 10% to viral pericarditis, 4% to Dressler’s syndrome and rare cases of tuberculosis, chest trauma, HIV, radiation to the mediastinum, hypothyroidism, and purulent pericarditis (Kabukeu).
In 20% of cases the etiology of the process is obscure.
Presentation may be nonspecific with dyspnea, chest pain, cough, weakness, fatigue, anorexia, and heart palpitations.
Small effusions may be asymptomatic.
When effusion accumulates to be hemodynamically significant cardiac tamponade symptoms appear.
Cardiac tamponade symptoms-Beck’s triad include triad, cyanosis, pulsus paradoxus, a positive Kussmaul’s sign and a pericardial rub.
Diagnosis suspected clinically and confirmed by echocardiography with right atrial and right ventricular collapse, dilated inferior vena cava with a lack of inspiratory collapse, and in extreme cases the heart oscillates within the pericardium.
Chest x-ray may show water bottle heart.
Many cases are first noted on abnormal CT chest studies.
Small effusions do not require treatment, but may improve with treatment of the underlying process such as the use of dialysis in renal insufficiency.
When effusion causes hemodynamic process urgent surgical removal of the pericardial fluid is required.
Removal of pericardial fluid may be achieved by pericardiocentesis, placement of a subxiphoid pericardial window, left anterior thoracostomy with pericardial window, video assisted thoracoscopic pericardiectomy (VATS) and median sternotomy with pericardiectomy.
Subxiphoid pericardial window is the procedure of choice form most patients and has minimal morbidity, and can prevent recurrence of tamponade in 97% of patients (Moores).
Pericardial windows require a 4 x 4 cm opening to be placed in the pericardium and tissue is submitted for pathological analysis, and pericardial tubes are placed to continue drainage.
VATS has better long term control of effusion compared to subxiphoid procedure, but requires pericardiocentesis must be performed prior to surgery.
Malignant involvement of the pericardium can manifest as pericarditis, pericardial effusion, pericardial tamponade or a pericardial constriction
Approximately 4-7% of patients presenting with pericarditis without a known malignancy will have a malignant pericardial effusion.
Pericardial effusion manifests in 20% of cases of malignancy.
Malignant pericardial involvement is detected during autopsy in1 to 2% of cases.
The most common malignancies involving the pericardium are lung cancer, breast cancer esophageal cancer, melanoma, lymphoma , and leukemia.