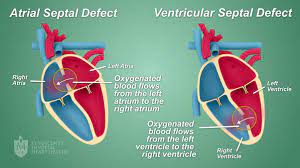
 Refers to a clot moving from the right side of the heart to the left through a patent foramen ovale, an atrial septal defect, or ventricular septal defect.
Refers to a clot moving from the right side of the heart to the left through a patent foramen ovale, an atrial septal defect, or ventricular septal defect.
Where it can enter the arterial circulation and possibly the brain.
Passage of a blood clot through a patent foramn ovale can be increased by a Valsalva maneuver and by a pulmonary embolism with elevated pulmonary arterial pressure.
An impending paradoxical embolism refers to a blood clot wedged between the opening of the atria or between the ventricles.
Patent foramen ovale seen in 15-35% of people, but paradoxical embolism is rare.
The risk of paradoxical embolism (ROPE) score incorporates, clinical characteristics-age, history of stroke, or TIA, diabetes, hypertension, smoking, cortical infarct on imaging to predict the likelihood that emboloc stroke of undetermined source was caused by a PFO.
More than 90% present with pulmonary embolism.
Systemic emboli such as cerebrovascular accident or peripheral vascular ischemia is documented in 55% of cases.
Okay, clinical factors not included.
DVT is noted in 22%.
30 day mortality rate greater than 18%, with many deaths occurring within 24 hours of diagnosis.
Shock, vascular collapse, coma and systemic embolization more common among nonsurvivors than survivors.
Systemic embolism most frequently related to the cerebrum with TIAs or ischemic strokes.
Transesophageal echocardiography is required for the diagnosis of pending paroxysmal embolism and is the test of choice.
Impending paradoxical embolism is associated with a high risk for morbidity and mortality, and is an emergency requiring rapid diagnosis and treatment.
The best treatment has not been defined and may vary between individuals: surgery thrombolysis, anticoagulation or a combination of treatments may be required.
Variables in the consideration of therapy includes the patient’s clinical presentation, existence of comorbidities, the presence of hemodynamic instability, clot size, risk for bleeding, and risk for systemic embolization.
Other potential risk factors for paradoxical embolism include:
Valsalva at stroke onset, recent prolonged travel, sleep apnea, presence of deep deep vein thrombosis or pulmonary embolism at presentation, hypercoagulability, migraine and other anatomical features such as a Chiari network.
Thromboembolectomy and closure of the patent foremen ovale or atrial septal defect are the favored management over thrombosis or anticoagulation.