 Page kidney or Page phenomena is a potentially reversible form of secondary arterial hypertension caused by external compression of the renal parenchyma by some perirenal process: Hematomas, urinomas, tumors, cysts, lymphoceles, and aneurysms have been reported.
Page kidney or Page phenomena is a potentially reversible form of secondary arterial hypertension caused by external compression of the renal parenchyma by some perirenal process: Hematomas, urinomas, tumors, cysts, lymphoceles, and aneurysms have been reported.
Compression is believed to cause activation of the renin–angiotensin–aldosterone system (RAAS) via microvascular ischemia.
Risk factors:
Renal biopsies and other medical procedures, contact sports, motor vehicle collisions.
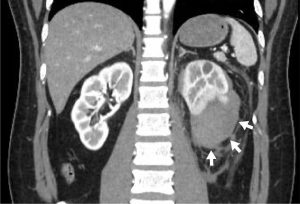
Diagnostic method is ultrasound, CT.
It is primarily a unilateral process.
In patients with only one solitary functioning kidney, the acute hypertension will also be accompanied by an acute decrease in renal function, therefore a prompt diagnosis and surgical treatment are needed to prevent irreversible kidney damage and restoration of kidney function.
Medical treatment involves use of an angiotensin-converting enzyme inhibitor (ACEi) or an angiotensin receptor blocker (ARB) to control the hypertension.
Causes of Page kidney have appeared to change over time: previously most often caused by traumatic injuries, such as contact sports or motor vehicle collisions, but more recently, the majority of cases are postprocedural or secondary to mass lesions.
Documented iatrogenic causes include: intra-abdominal surgery, lithotripsy, renal biopsy, and percutaneous endopyelotomy.
Kidney allograft biopsy accounts for the majority of Page kidney cases.
The activation of the renin–angiotensin–aldosterone system (RAAS) is caused by the compression of the renal parenchyma altering intrarenal blood flow, resulting in a localized decrease in blood flow to the affected nephrons.
This decrease in blood flow is recognized by the juxtaglomerular (JG) cells and promotes the cleavage of prorenin into renin.
Kidneys are surrounded by two layers of connective tissue, the inner renal capsule and outer renal (Gerota’s) fascia, forming two potential spaces where fluid can form, the small subcapsular space and the large perinephric space.
Because the renal capsule is fibrous and does not easily expand, a small collection of blood in the subcapsular space can cause mass pressure effect on the renal parenchyma.
Diagnosis of Page kidney is based on imaging studies:
abdominal x-ray, intravenous pyelography, angiography, renal doppler ultrasound, CT scan, and MRI).
Diagnosis is primarily made by ultrasound and CT, identifying the mass like lesion.
Doppler ultrasound is needed to display the hemodynamic changes occurring in the kidney.
Treatment:
Historically open surgery nephrectomy was performed, now replaced by less invasive percutaneous drainage or endoscopic capsulotomy.
Some cases resolve spontaneously without need for surgical treatment, and can be managed by medical treatment with an angiotensin-converting enzyme inhibitor (ACEi) or an angiotensin receptor blocker (ARB).
Adding a calcium channel blocker (CCB) or beta blocker to the ACEi or ARB has been efficacious.