 Syndrome characterized by urinary urgency, with or without urgency urinary incontinence, usually with increased frequency day or night.
Syndrome characterized by urinary urgency, with or without urgency urinary incontinence, usually with increased frequency day or night.
Overactive bladder detrusor affects approximately 16% of men in the US.
Defined as urinary urgency, usually accompanied by frequency and nocturia with or without urinary incontinence in the absence of pathologic or metabolic conditions that might explain these symptoms.
Urinary urgency is the most defining feature of OAB.
Can negatively impact social, psychological, occupational, domestic, physical and sexual functioning.
One definition of an overactive bladder is when a person urinates more than eight times per day.
0AB-dry sometimes used to refer to women with urgency-frequency without urge incontinence.
OAB-wet refers to women with urging incontinence associated with wetting accidents.
An overactive bladder can often cause urinary incontinence.
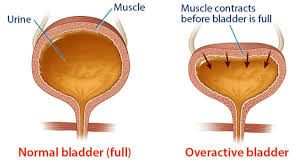
Specific cause for OAB is not known, but is thought to result from an inappropriate contraction of the detrusor muscle.
In the majority of women the syndrome is idiopathic.
Often attributed to detrusor overactivity associated with involuntary detrusor contractions during bladder filling.
In men may coexist with bladder outlet obstruction due to BPH, or secondary to obstruction whereby increased pressure required to void leads to bladder structural changes causing detrusor smooth muscle excitability.
Estimated 10 million men 40 years or older have symptoms.
Prevalence over the age of 40 years is 16.6%.
Affects up to 20% of US adults
From 9-43% of women worldwide are affected.
Maybe associated with the number neurologic conditions including multiple sclerosis, stroke, and Parkinson’s disease.
Prevalence in severity of symptoms increases with age.
Women with obesity you have a much higher risk of developing urge incontinence compared with women without obesity.
A dose response relationship exist between body mass index and the risk of urinary incontinence.
Non- neurogenic overactive bladder (OAB) in adults diagnosis requires a thorough history, physical exam, and urinalysis.
A urine culture and/or postvoid residual assessment may be necessary.
Urodynamics, cystoscopy, and diagnostic renal and bladder ultrasound are not necessary are reserved for refractory or otherwise complicated cases.
Treatment includes behavioral therapies such as bladder training, bladder control strategies, pelvic floor muscle training, and fluid management.
Antimuscarinics are second-line therapy.
Extended-release preparations are preferred over immediate-release preparations to limit dry mouth.
Transdermal oxybutynin patches or gel can also be used.
Antimuscarinics should not be used by patients with narrow-angle glaucoma, and used with caution in patients with impaired gastric emptying or who have a history of urinary retention.
Attempts should be made to manage constipation and dry mouth before discontinuing antimuscarinics agents.
Caution must be used in patients taking other medications with anticholinergic properties.
Nearly 80% of patients discontinue use of antimuscarinics at a mean of 4.8 months.
Sacral neuromodulation is a third-line treatment to patients with refractory overactive bladder symptoms.
Peripheral tibial nerve stimulation (PTNS) using an acupuncture needle, can provide benefits for patients with moderately severe incontinence and frequency.
Indwelling catheters are not recommended for management because of risks.
First line treatment for overactive bladder includes behavior modification, bladder training, and pelvic floor physical therapy.
Behavioral therapies are as effective as pharmacologic therapy.
Fluid restriction is a key component of behavioral modification.