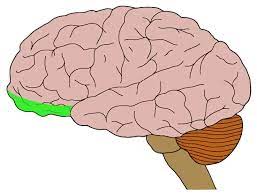
The orbitofrontal cortex (OFC) is a prefrontal cortex region in the frontal lobes of the brain which is involved in the cognitive process of decision-making.
It is the area of the prefrontal cortex that sits just above the orbits.
It is thus found at the very front of the brain, and has extensive connections with sensory areas as well as limbic system structures involved in emotion and memory.
It consists of Brodmann area 10, 11, 12, 13, and 47.
It is part of the frontal lobe.
It is considered anatomically synonymous with the ventromedial prefrontal cortex.
As part of the prefrontal cortex that receives projections from the medial dorsal nucleus of the thalamus: represents emotion, taste, olfaction and reward in decision making.
It is immediately above the orbits in which the eyes are located.
It has four gyri are split by a complex of sulci.
The caudal OFC is more heavily interconnected with sensory regions, receiving direct input from the pyriform cortex, and is the most heavily interconnected with the amygdala.
Rostrally, the OFC receives fewer sensory projections, and is less connected with the amygdala, but it is interconnected with the lateral prefrontal cortex and parahippocampus.
The OFC receives projections from multiple sensory modalities: olfactory cortex, gustatory cortex, secondary somatosensory cortex, superior and inferior temporal gyrus conveying visual information all project to the OFC.
The OFC also receives input from the medial dorsal nucleus, insular cortex, entorhinal cortex, perirhinal cortex, hypothalamus, and amygdala.
The orbitofrontal cortex is reciprocally connected to: the perirhinal and entorhinal cortices, the amygdala, the hypothalamus, and parts of the medial temporal lobe.
The OFC also projects to the striatum, including the nucleus accumbens, caudate nucleus, and ventral putamen, as well as regions of the midbrain including the periaqueductal grey, and ventral tegmental area.
OFC inputs to the amygdala synapse on multiple targets.
Functions ascribed to the OFC including: mediating, encoding contingencies in a flexible manner, encoding value, encoding inferred value, inhibiting responses, learning changes in contingency, emotional appraisal, altering behavior through somatic markers, and driving social behavior, encodes state spaces, the discrete configuration of internal and external characteristics associated with a situation and its contingencies.
The OFC responds to a diverse tasks, and is capable of rapidly remapping during contingency shifts.
The OFC is necessary for ventral tegmental area (VTA) neurons to produce a dopaminergic reward prediction error, and the OFC may encode expectations for computation of RPEs in the VTA.
The lateral OFC supposedly reflects potential choice value, enabling switching choices during reversal, extinction and devaluation.
The medial OFC responding most often to reward, and the lateral OFC responding most often to punishment.
The posterior OFC responds to more simple reward, and the anterior OFC responds more to abstract rewards.
The OFC and basolateral amygdala are highly interconnected.
The posterior orbitofrontal cortex is connected to the amygdala by multiple paths, capable of both upregulating and downregulating autonomic nervous system activity.
The neuromodulator dopamine plays a role in mediating the balance between the inhibitory and excitatory pathways, with a high dopamine state driving autonomic activity.
It is suggested that the medial OFC is involved in making stimulus-reward associations and the reinforcement of behavior.
The lateral OFC is involved in stimulus-outcome associations and the evaluation and possibly reversal of behavior, and encode new expectations about punishment and social reprisal.
The mid-anterior OFC tracks subjective pleasure in neuroimaging studies.
The anterior OFC, is capable of enhancing liking response to sucrose.
The OFC can modulate aggressive behavior via projections to the amygdala that inhibit glutaminergic projections to the ventromedial hypothalamus.
Electrophysiologically neurons in the OFC respond both to primary multiple sensory domains of visual, gustatory, somatosensory, and olfactory stimuli.
Evidence for auditory responses are weaker.
Neural responses in the OFC to rewards or reward cues are modulated by preferences and by motivational states such as hunger.
A fraction of neurons that respond to sensory cues predict a reward or are selective for reward, and exhibit reversal behavior when cue outcome relationships are swapped.
Neurons in the OFC also exhibit responses to the absence of an expected reward, and punishment.
OFC fires in response to cues; firing before rewards ; firing in response to rewards.
OFC neurons do not exhibit firing mediated by movement.
OFC reward-predictive responses are shaped by attention:the OFC population represents positively the value of a currently attended item, but negatively the value of the unattended item.
It is suspected that OFC is involved in sensory integration, in representing the affective value of reinforcers, and in decision-making, expectation, and in signaling the expected rewards/punishments of an action given the particular details of a situation.
The OFC of the brain is capable of comparing the expected reward/punishment with the actual delivery of reward/punishment, thus, making it critical for adaptive learning.
The orbitofrontal cortex dysfunction has been implicated in borderline personality disorder, schizophrenia, major depressive disorder, bipolar disorder, obsessive-compulsive disorder, addiction, post-traumatic stress disorder, Autism, and panic disorder.
The OFC’s anatomical connections with the ventral striatum, amygdala, hypothalamus, hippocampus, and periaqueductal grey support a role in mediating reward and fear related behaviors.
Neuroimaging studies in OCD report hyperactivity in areas generally considered to be part of the orbitofrontal segment of the cortico-basal ganglia-thalamo-cortical loop such as the caudate nucleus, thalamus and orbitofrontal cortex.
The OFC is usually overactive during symptom provocation tasks, and cognitive tasks usually elicit hypoactivity of the OFC.
Substance use disorders are associated with a variety of deficits related to flexible goal directed behavior and decision making, which overlap with symptoms related to OFC lesions, and are also associated with reduced orbitofrontal grey matter, resting state hypometabolism, and blunted OFC activity during tasks involving decision making or goal directed behavior.
Cues associated with drugs evoke robust OFC activity that correlates with craving.
Dysfunction in the OFC, like that produced by drugs of misuse, could underlie drug seeking habits.
Abnormalities in OFC structure, activity, and functional connectivity are observed in association with aggression.
Neuroimaging studies have found abnormalities in the OFC in major depression disorder and bipolar disorder.
Hypoactivity of the lateral OFC has been frequently observed in bipolar disorder, in particular during manic episodes.
Some neuroimaging studies have observed elevated lateral OFC activity in depression, as well as reduced interconnectivity of the medial OFC,
Destruction of the OFC through acquired brain injury typically leads to a pattern of disinhibited behavior: swearing excessively, hypersexuality, poor social interaction, compulsive gambling, drug use and poor empathizing ability.
Disinhibited behavior with some forms of frontotemporal dementia may be caused by degeneration of the OFC.
The main disorders associated with dysregulated OFC connectivity/circuitry center around decision-making, emotion regulation, impulsive control, and reward expectation.
A disrupted structural and functional connectivity of the OFC with the subcortical limbic structures of the amygdala or hippocampus and other frontal regions of the dorsal prefrontal cortex or anterior cingulate cortex, correlates with abnormal OFC affect processing in clinically anxious adults.
Problems with decision-making as in drug addiction/substance dependence, can result from disruption of the striato-thalamo-orbitofrontal circuit.
Attention deficit hyperactivity disorder (ADHD) has also been implicated in dysfunction of neural reward circuitry controlling motivation, reward, and impulsivity, including OFC systems.
Executive functioning and impulse control may be affected by OFC circuitry dysregulation: obsessive–compulsive disorder and trichotillomania.
Some dementias are also associated with OFC connectivity disruptions.
Frontotemporal dementia is associated with neural atrophy patterns of white and gray matter fibers involved with OFC connectivity.
The later stages of Alzheimer’s Disease be impacted by altered connectivity of OFC systems.
Orbitofrontal epilepsy is rare, and its characteristics include sleep related symptoms, automatisms, and hypermotor symptoms.
Patients with OFC dysfunction cannot judge when something socially awkward has happened.