 Refers to thickened skin seen in prolonged hypothyroidism.
Refers to thickened skin seen in prolonged hypothyroidism.
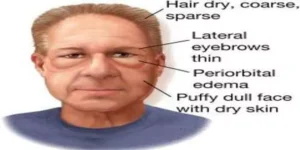
Myxedema refers to severe hypothyroidism.
The term also refers to deposition of mucopolysaccharides in the dermis, which results in swelling of the affected area.
It is a specific form of cutaneous and dermal edema secondary to increased deposition of connective tissue components.
Pretibial myxedema also refers to a skin condition affecting the shins in some patients with Graves’ disease.
Pretibial myxedema, a hallmark of Graves disease, an autoimmune form of hyperthyroidism.
Myxedema can also occur in Hashimoto thyroiditis and other long-standing forms of hypothyroidism.
Severe cases, requiring hospitalization can exhibit signs of hypothermia, hypoglycemia, hypotension, respiratory depression, and coma.
Myxedema is more common in women than in men.
Myxedema can occur in:
Hyperthyroidism, associated with pretibial myxedema and exophthalmos.
Pretibial myxedema can occur in 1–4% of patients with Graves’ disease, a cause of hyperthyroidism.
The connective fibers are separated by protein and mucopolysaccharides: including glycosaminoglycans, such as hyaluronic acid, chondroitin sulfate and other mucopolysaccharides.
Then protein-mucopolysaccharide complex binds water, producing the non-pitting boggy edema, seen around eyes, hands, feet and in the supraclavicular fossae.
Myxedema is responsible for the thickening of the tongue and the laryngeal and pharyngeal mucous membranes, causing slurred speech and hoarseness, both of which are seen commonly in hypothyroidism.
It is suspected fibroblast stimulation by the thyroid stimulating hormone (TSH) receptor increases the deposition of glycosaminoglycan.
Suspected that many cells responsible for forming connective tissue react to increases in TSH levels.
Increased glycosaminoglycan results in an osmotic edema and tissue fluid retention.
In Graves’ disease, lymphocytes react against the TSH receptors by inappropriately producing thyroid-stimulating immunoglobulin (IgG; type II hypersensitivity reaction) , and other tissue with cells expressing the receptor leading to tissue damage and scar tissue formation, explaining the deposition of glycosaminoglycans.
Myxedema can be diagnosed on clinical grounds alone.
Characteristic findings:weakness, cold intolerance, mental and physical slowness, dry skin, typical facies, and hoarse voice.
The total serum thyroxine and free thyroxine index tests usually will confirm the diagnosis.
Treatment is the administration of adequate doses of either the thyroid hormone L-thyroxine given intravenously or by giving liothyronine via a nasogastric tube.
((Myxedema coma)) is rare but often fatal.
Myxedema coma occurs most often in elderly women.