 Clonal hematopoietic stem cell disorders characterized by ineffective hematopoiesis and peripheral cytopenias.
Clonal hematopoietic stem cell disorders characterized by ineffective hematopoiesis and peripheral cytopenias.
Criteria for diagnosis of MDS consist of anemia, thrombocytopenia, or neutropenia that persist for six months or longer, dysplasia greater than 10% in at least one bone marrow cell lineage, and MDS associated clonal cytogenetic abnormalities or molecular markers.
Conditions associated with bone marrow failure such as aplastic anemia with hypocellular marrow, typical bone marrow findings of MDS are a hypercellular marrow for a persons age, dysplasia in 1 to 3 lineages manifested by pseudo Pelger-Huet nuclei, hypogranular neutrophils, micro megakaryocytes, and/or ringed sideroblasts, glass Siri glass, and increased myeloblasts in a subset of patients.
In patients with unexplained anemia, thrombocytopenia, or neutropenia without dysplasia in the bone marrow but with abnormal chromosome activity in 5, 7 or 13 the diagnosis is consistent with MDS and occurs in less than 10% of patients with MDS.
There is clonal proliferation of malignant hematopoietic stem cells, dysregulated cellular differentiation, and compromised tissue function.
Iincidence is approximately 4.5 per 100,000 people.
It is rare among children, and accounts or 1.6% of cases below age 40.
Growth and spread of a somatically mutated clone is the pathological process that leads to MDS.
The clone has a advantage provided by the somatic genetics change with driver mutations.
The mutation occurs in hematopoetic stem cells capable of self renewal and additional mutations are associated with clonal progression may occur in progenitor cells conferring a self renewal capability.
More than 90% of cases of MDS harbor detectable drive mutations including: DNMT3A, EZH2, RUNX 1, TET 2, IDH 1, IDH 2, TP53, ASXL1, and mutations in genes in coding components involved in the three prime RNA splicing.
Mutation-driver genes cause clonal outgrowth and propagation of myelodysplastic hematopoiesis.
Most patients with myelodysplastic syndrome have greater than one mutation and a unique pattern of mutation with marked heterogeneity.
Adverse mutations are present in approximately 20% of patients with very low risk MDS with a median survival nearly one third shorter than that have low-risk patients without these mutations.
For patients with low and intermediate IPSS risk, mean overall survival was approximately 50% shorter compared with those without mutations.
Patients with the greater number of somatic mutations have inferior overall survival.
Somatic mutation is not a static process in myelodysplastic syndrome and additional mutations will accumulate leading to more profound phenotypic worsening cytopenias, and approximately 30% of patients will eventually experience progression to secondary AML.
When the bone marrow hematopoietic cells are mostly clonally derived cells, the disease is clinically manifested as cytopenia and morphologic dysplasia.
The paradox is that the mutation provides advantage at the stem cell level and progenitor cells, with a disadvantage at the level of hematopoietic precursors.
The clonal outgrowth of mutant stem cells favors and abnormal hematopoietic stem cell niche.
Patients with myelodysplastic syndromes (MDS) collectively have a high symptom burden and are also at risk of death from complications of cytopenias and acute myeloid leukemia.
The incidence of MDS in the United States increases exponentially from age 40 where the rate is 0.2 per 100,000 people, to age 85 where there are 45 cases of MDS per 100,000 people.
Crude incidence 4-5 cases per hundred thousand persons per year.
The yearly incidence rate increases to 25 per hundred thousand people age 65 years or older.
Old age is associated with clonal hematopoiesis of indeterminate potential which is considered a precursor to MDS.
Most prevalent in older adults, with the median age at diagnosis ranging between age 70 and 75 years.
Currently there are approximately 10,000 to 15,000 new cases of MDS diagnosed annually in the United States.
It is rare among children, adolescents, and young adults.
The incidence is believed to be increasing.
More common in men with a yearly incidence rates of approximately 5.4 per hundred thousand versus 2.9 per hundred thousand for women.
It is more common among people who are White as compared with people who were Asian/pacific islander, Black or Hispanic and among people who are older.
With the aging of the US population, the incidence of MDS and AML are likely to increase.
Acquired, irreversible group of clonal disorders.
Most common cause of acquired bone marrow failure in adults.
Characterized by dysplastic and ineffective blood cell production and cytopenias despite a hypercellular bone marrow.
Foundation for diagnosis relies on the morphological dysplasia involving one or more cell lines and ineffective clonal hematopoiesis that result in peripheral blood cytopenias.
Subcategorized as primary, de novo or secondary as arising from previous chemotherapy, radiation therapy, or antecedent myeloid malignancy.
Risk factors include prior exposure to chemotherapy or radiation therapy, antecedent hematologic conditions such as aplastic anemia or paroxysmal nocturnal hemoglobinuria, autoimmune disorders such as rheumatoid arthritis, environmental exposures to toxin such as organic solvents, and congenital predisposition syndrome such as Fanconi‘s anemia or germline variants in hematopoetic stem cells.
Subtypes are diagnosed on the basis of the number of dysplastic lineages, presence or absence of ring sideroblasts, percentage of bone marrow and peripheral blood blasts, and type of cytogenetic abnormality.
Inherently volatile and can transform into acute myelogenous leukemia.
Hypercellularity of bone marrow is a result of increased a apoptosis in the bone marrow.
Pathophysiology remains elusive with the only exception of del(5q), in which haploinsufficiency of ribosomal gene RPS14, which is required for the maturation 40S ribosomal subunits and maps to the deleted region, and homozygous inactivation of the casein kinase 1A1 gene (CSNK-1A1) play a central role in disease.
MDS associated with chromosomal lesion del(5q) with losses that span 5q31-q33 and occur in isolation often exhibit macrocytic anemia, thrombocytosis, hypolobated micromegakaryocytes, and a relatively indolent course.
Anemia is the most frequent presentation and is often progressive and ultimately results in red blood cell transfusion dependency.
Leukopenia or thrombocytopenia associated symptoms may be present.
Patients may present with recurrent bacterial infections due to neutropenia in approximately 2 to 50% of patients.
Anemia is the main cause of morbidity in myelodysplastic syndrome and is often blamed for symptoms of fatigue and other constitutional symptoms.
MDS patients with an isolated del(5q) and lower risk of transfusion dependence, have a favorable response to lenalidomide: response rates of 50 to 80%, which are deep and durable:these patients on average, have responses lasting greater than 1 1/2 years, and in many exceed two years.
Lenalidomide works through a defect in ribosomal protein function via ubiquitination and degradation of casein 1A.
Lenalidomide reduces transfusion requirement in approximately 1/4 of patients without del(5q), although responses are generally of shorter duration than hypomethylating agents.
A small number of patients with low-risk disease, less than 5% blasts in the bone marrow and age less than 60 years will respond to T-cell mediated immunosuppressive therapy including antithymocyte globulin, cyclosporine or tacrolimus.
The presence of hypoplastic disease and HLA-DR15 predict a higher likelihood of response to immunosuppressive therapy.
Immunosuppressive therapy in low-risk disease is considered after failure to respond to erythrocyte stimulating agents.
Excessive intramedullary apoptosis of hematopoietic progenitors and more mature cells, mediated by cytokines such as tumor necrosis factor, interleukin-1 beta and transforming growth factor beta.
Elevated concentrations of cytokines in the bone marrow and plasma of patients.
In early disease the interaction between the myelodysplastic clone and the microenvironment of the bone marrow releases agnogenic and inflammatory molecules that lead to unrestrained cellular proliferation and apoptotic cell loss referred to as ineffective hematopoiesis.
A consequence of abnormal regulation in cellular survival and differentiation affecting proliferation, apoptosis, and differentiation of hematopoietic progenitors.
The disease causing mutation is currently unknown, but the phenotype of MDS is affected by secondary mutations, haploinsufficiency, epigenetic changes and altered responses resulting in cytokine, immune and bone marrow stromal changes (Tefferi A et al).
Epigenetic mechanisms may alter transcription of tumor suppressive genes and lead to clonal expansion and disease progression in myelodysplastic syndrome.
Likely all MDS patients have 1 or more somatic driver mutations related to the development of the disease and its progression.
Associated with increased genomic instability.
When cytogenetics studies are combined with gene sequencing, 90% or more of patients with MDS carrier clonal genetic lesion.
Apoptosis predominates in early stages and proliferation may increase in later stages and exceed apoptosis.
Signals form NF-kB, Bcl-2, Bcl-X Bim-1, and phospho-Akt may upregulate cellular survival and heat shock proteins suppress apoptosis and propagate the malignant clone.
The erythroid progenitor response to EPO may be modestly depressed, but excessive apoptosis is associated with overexpression of fas ligand undermining differentiation.
Excess inflammatory cytokines in the micro environment of the bone marrow amplifies defects in erythroid maturation and decreases erythroid survival.
There is a complex interplay between apoptotic cytokines and autocrine production of antigenic molecules, such as VEGF, reinforcing the malignant phenotype.
Abnormal silent sitting of tumor suppressive and DNA repair genes which are mediated by hypermethylation of their promoters have an important role in the pathogenesis.
DNA repair defects probably related to chromosomal instability and repetitive chromosomal defects in MDS.
T cells from patients with MDS inhibit granulopoiesis and erythropoiesis suggesting an immune mediated suppression of hematopoiesis.
Increased bone marrow neovascularization present in MDS.
Dysplasia of at least one bone marrow lineage is characteristic.
Vitamin B 12 and folate deficiency, HIV or other infections, alcohol abuse, medication such as methotrexate and chemotherapy, copper deficiency, autoimmune disorders and large granular lymphocyte disorders, Fanconi Syndrome and even aplastic anemia and myeloprolferative disorders must be distinguished.
Bcl-2 and other oncoproteins are involved in programmed cell death in myelodysplasia.
Median age 7O years at diagnosis..
The incidence rate is 0.22/100,000 in individuals younger than 49 years, 4.8/100,000 between ages 50 and 70 years and 22.8/100,000 in those older than 70 years.
Men affected more often than women 2.3:1.
Has genetic and morphologic heterogeneity and can vary in its natural history and prognosis.
Affects approximately 55,000-76000 patients in the U.S.
The incidence in the US increases exponentially from age 40 with the rate is 0.2 per hundred thousand people, to age 85 with 45 cases per 100,000 people.
Approximately 15-20,000 cases per year.
Annual incidence in the general population is about 5 per 100,000.
One of the most frequent hematologic cancers raffecting the elderly, with an annual incidence rate exceeding 50 cases per hundred thousand in persons age 65 years or older
Survival can be limited to a few months in symptomatic patients, whereas others with minimal symptoms can survive for decades.
The incidence is approximately 8 per 100,000 between ages 60 and 70 years and greater than 20 per hundred thousand after age 70 years.
Approximately 86% of patients are diagnosed after the age of 60 years.
Increase of incidence to 20 per 100,000 to 50 per 100,000 in people older than 60 years.
Rare in young people with an estimated incidence of less than one per hundred thousand before age 50 years and approximately 2 per hundred thousand between ages 50 and 60 years.
Occurrence before the age of 50 accounts for only 6% cases.
Men have a higher incidence.
Whites have a higher incidence then do other ethnic groups.
Estimated that at least 15,000 new cases diagnosed each year in the U.S.
May be as many as 45000 cases per year in the US (Goldberg SL et al).
May be more prevalent than estimation due to underdiagnosing and undereporting.
Based on Medicare billing annual incidence may be 7-8 times higher than reported (Goldberg SL).
Approximately 50% of patients have clonal cytogenetic abnormalities and 50% have normal cytogenetics.
Diagnosis requires bone marrow examination and cytogenetic studies with minimal criteria for diagnosis in the presence of erythroid, granulocytic, or megakaryocyte dysplasia in 10% or more of cells.
Bone marrow by definition has less than 20% of blasts.
Differential diagnosis includes erythroid dysplasia from vitamin B12/folate/copper deficiencies, viral infections, chemotherapy, or lead/arsenic poisoning.
Up to 80% of patients with secondary myelodysplastic syndrome have karyotypic abnormalities.
More than 40 mutated genes identified in MDS.
Mutations occur in several oncogenes and tumor suppressor gene including: NRAS, JAK2, TP53, FMS, TET2, IDH AND EZH2.
Germline mutations in RUNX1, TET2, c-CBL, and ASXL1 have also been identified in MDS.
Mutations in ASXL1, RUNX1, ETV^, EZHZ, or TP53 have a higher risk of progression of disease.
Splicing factor genes SF3B1, SRSF2, U2AF1, and ZRSR2 are present in more than 12% of MDS patients, an are associated with prognostic significance (Thol F et al).
SF3B1 mutations related to subtype refractory anemia with ringed sideroblasts, Ineffective erythropoiesis, and macrocytic anemia and is associated with improved prognosis: most patients become transfusion dependence, and co-mutations are associated with a worst outcome.
SRSF2 and U2AF1 splicesome genes are mutated in various myeloid neoplasms and generally characterized by poor clinical outcome.
With exception of TET2 most above genes are mutated in no more than 5-15% of cases.Mutations are less frequent in the more benign subtypes of the disease.
ASXL1 gene mutation found in 11% f patients with MDS, and predicts for an adverse outcome.
Epigenetic modifications, including apparent DNA methylation has also been noted to be present in MDS.
Most cases of unknown etiology.
Most cases are de novo.
Originates from somatic mutations, not yet specified, affecting hematopoetic stem cell and resulting in clonal myelopoiesis that is morphologically dysplastic and functionally ineffective.
About 10% of MDS patients have secondary or therapy related disease.
Prognosis in secondary disease is poorer than those with de novo disease, and they have more complex cytogenetic abnormalities.
It is expected that patients with secondary MDS will increase due to chemotherapy and radiation usage.
Median time to development following chemotherapy 4-5 years.
Therapy related myelodysplasia and acute myelogenous leukemia after high-dose chemotherapy is between 5% and 15%.
Initiated by toxins including pesticides, cotton and flax dust, organic solvents, radiation, chemotherapy, metals, asbestos and cigarette smoking.
A significant linear radiation dose response for MDS he exists in atomic bomb survivors 40-60 years after radiation exposure and all patients following irradiation should have long term followup (Iwanaga M et al).
Both environmental and therapeutic exposure to radiation increase the risk of secndary MDS.
The effect of radiation on MDS risk is greater in advanced subtypes of MDS and and does expose that younger ages ((Iwanaga M et al).
Approximately 71% of newly diagnosed patients have lower risk disease.
Approximately 29% of newly diagnosed cases have higher risk disease with a median expected survival time < 2 years.
A recent study suggested a median survival estimated at 2.5 years and has not improved over the past several decades, with the most common causes of death progression to AML, 47%, infections 27%, and bleeding 10%.
5 year survival is approximately 37%.
The evolution to AML is a process of clonal selection.
Mutations driving leukemic transformation may be present at the onset of disease but only expand later.
Transformation to AML occurs with different patterns depending upon the mutations present, or acquired, and if there are combinations of mutated genes.
Gene predisposition disorders collectively account for up to 15% of all cases of MDS, and detecting the germline mutation is important for genetic counseling and also for clinical decision making.
Good risk patients have a median survival of 5.7 years, while poor risk patients have a median survival of 0.4 years.
Three year survival rates estimated at less than 50% (Rollinson DE et al).
The patients who have the worst prognosis are those with the lowest blood counts, the most cytogenetic abnormalities and with the highest number of blasts in the bone marrow.
Elevated levels of tumor necrosis factor-alpha and cytotoxic T-cells can lead to ineffective hematopoiesis in some cases, suggesting immunosuppressive therapy may be of benefit.
Patients that require red blood cell transfusions have the poorest prognosis.
Red blood cell transfusion requirement is an independent variable adversely affecting survival in patients with lower risk disease.
The total number of red blood cell transfusions and transfusion frequency as administered per month associated with a proportional decline in overall survival and in leukemia fee survival (Malcovati).
Risk is divided into groups on the basis of the International Prognostic Scoring System (IPSS) criteria.
The revised IPSS scoring system IPSS-R is most commonly used risk stratificarion and disease classification scheme.
All scoring systems incorporate the depth and number of cytopenias present, the burden of myeloid blasts cells found in the bone marrow or blood, and the genetic composition via cytogenetic analysis.
The IPSS-R utilizes five cytogenetic risk categories and clinical variables including bone marrow blast percentage, hemoglobin level, platelet count, absolute neutrophil count with median survivals ranging in the five risk categories from 0.8-8.8 years.
Risk groups are based on whether patients are untreated or received growth factor support, providing insight to prognosis.
Low risk groups of those with IPSS low and intermediate-1 scores and high-risk of those with IPSS intermediate-2 and high-scoring spirit.
Estimated at 39% of patients with low-and intermediate-1 risk patients will require red blood cell transfusions on a regular basis and thus her risk for complications iron overload.
Diagnosis suspected with unexplained anemia associated with other cytopenias, increased MCV or increased red cell distribution width.
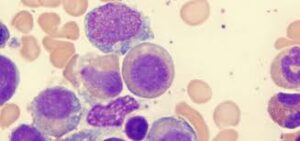
Peripheral blood smear reveals oval macrocytes, dimorphic red blood cells, hypo segmented and hypogranulated neutrophils.
During a three year follow-up of patients with MDS and iron overload those patients that received red blood cell transfusions expeienced more cardiac complications more frequently than those who did not receive transfusions (Goldberg SL).
Nonleukemic causes of death associated with transfusion need in such patients.
RBC transfusion dependence is associated with a 36% reduction in survival for every 500 mcg/L increase in serum ferritin above 1000 mcg/L.
Patients may have iron toxicity after receiving as few as 20 uits of red blood cells (Porter JB).
Baseline transfusion dependence and iron overload are independent prognostic variables for overall survival at the time to progression to acute myelogenous leukemia.
Patients with myelodysplastic syndrome and transfusion dependence have more than a twofold higher risk of death and 6 old higher risk of leukemic transformation compared with patients without such transfusion requirement during the initial 3 years after diagnosis (Goldberg SL).
The negative prognosis associated with transfusion dependence is partially due to hemosiderosis and secondary organ damage.
Elevated iron levels in myelodysplastic syndromes increase risk of infection and leukemic progression by promoting bacterial growth and inducing genetic damage.
Chronic anemia is associated with cardiac mortality via cardiac remodeling as a result of long-term hemodynamic compensation.
MANAGEMENT:
Supportive care consists of blood transfusions, antibiotics, growth factor support and iron chelation therapy, and is the treatment of choice for a large percentage of the mostly elderly patients in this population.
No therapeutic intervention has been shown in a randomized clinical trial to improve overall survival compared with receiving no therapy for low risk disease.
Recommended treatment options for lower risk MDS include includes azacididine , decitabine, cedaxuridine or immuno suppressive therapy with without eltrombopag, hypomethylating agents, ivosidenib, allogeneic HCT.
Immunosuppressive therapy includes anti-thymocyte globulin with or without cyclosporine A.
Treatment consist of reducing disease related symptoms, lessening, or eliminating transfusions, minimizing, morbidity due to chronic anemia, thrombocytopenia, or neutropenia.
Treatment selection is dependent upon the predominant bone marrow abnormality of anemia, thrombocytopenia, or neutropenia.
Most patients with anemia have associated adverse events with cardiopulmonary and cognitive decline, increased risk of falls at a reduced overall survival.
Erythropoietic stimulating agents have a response rate of less than 40%.
Patients with the ring sideroblasts and anemia, and those with disease either refractory to ESA‘s or unlikely to respond to ESA, and can be treated with luspatercept.
Luspatercept is a recombinant fusion proteins that bind transforming growth factor B super family ligands to reduce SMAD2 and SMAD3=signaling in late stages of erythropoiesis.
The majority of patients with MDS become red cell transfusion dependent during their clinical course, and a hemoglobin level of 8 g of deciliter is generally used as a transfusion threshold.
The goals of therapy are to reduce disease-associated symptoms and the risk of disease progression and death.
Treatment is based on the type of MDS, MDS risk group, and other factors, as well as patient age and overall health.
Treatment options for patients with myelodysplastic syndromes (MDS) remain fairly limited and include: lenalidomide for patients with del (5Q) cytogenetic abnormalities, azacitidine, or decitabine, or the oral combinations of the decitabine and cedazuridine for treating higher risk MDS or MDS unnresponsive, deferoxamine and deferasirox for the treatment of iron overload, luspatercept for treating MVS with ring sideroblast in patients with no response to prior erythropoiesis stimulating agent or for treatment of lower risk MDS, Imetelstat for treating lower risk MDS, in patients with no response to ESAs or those who are eligible for ESA‘s and ivisidenib for patients with relapsed or refactory, mutant IDH1 MDS and allogeneic hematopoietic cell transplant (allo-HCT).
As patients are in their late 70s, about 40 to 50% of patients with MDS survive five years after transplantation.
Patients with somatic mutations in TP53 predicts for early relapse and shorter survival.
TP 53 is adverse in almost all settings, including patients who are undergoing transplantation: it is associated approximately 50% shorter long-term survival when compared with those without the mutation.
Patients who fail to respond to the standard of care, have an outcome that is dismal.
Therapy for low-risk disease focuses on mitigation of cytopenias and symptoms , whereas those employed for higher-risk disease seek to modify the natural history of disease.
In patients with indolent disease who do not have transfusional needs and with minimal symptoms monitoring may be the most appropriate approach.
Cardiac complications occur more frequently among patients with MDS than among the overall Medicare population.
MDS patients that receive transfusions experience cardiac complications more frequently than those MDS patients that do not receive such transfusions.
More MDS patients who receive transfusions have a higher likelihood of developing diabetes than those not receiving such transfusions.
Iron overload is associated with lower overall probability of survival.
Iron overload is associated with an increased AML transformation rate and decreased survival.
Studies have shown that combinations of G-CSF and erythropoietin versus erythropoietin alone have higher response rates in controlling anemia and can decrease red blood cell transfusion dependency.
Among unselected patients 15-30% will have a favorable erythroid response to recombinant human erythropoietin, and in selected patients with a favorable response profile 40-70% will respond.
In patients with low risk disease and limited red blood cell transfusion requirement growth factors can increase overall survival (Jadersten).
More than 70% of patients are above the age of 60 years.
May be the most common malignancy worldwide.
Prevalence in the U.S. is from 30-60,000.
Incidence of 1 in 500 patients over the age of 60 years.
Steadily increasing in incidence.
Likely diagnosis is underreported as elderly with mild anemia may not be evaluated because of other coexisting medical problems.
Most common hematologic malignancy in the elderly.
Incidence increases with age and estimated rate in patients over the age of 70 years is 15-50 cases/100,000 per year.
Median age at diagnosis is 70 years.
For all subtypes of disease family history of hematopoietic malignancy, exposure to agricultural chemicals and solvents associated with increased risk.
Bone marrow is hypercellular in most cases.
10-20% of patients have a hypocellular bone marrow that is present at the outset or evolves as the disease progresses.
Originates in the pluripotent stem cell line.
High proliferation disorder with high degree of apoptosis and intramedullary cell death.
More than 70% of bone marrow cells undergo cell death.
Anemia most common presenting factor, in 85% of patients.
68% of patients with higher-risk disease are dependent on RBC transfusions and 33% require platelet transfusions (Sekeres MA).
20-30% of cases evolve into acute leukemia.
French-American-British (FAB) Cooperative Study Group defined 5 subtypes based on percentage of immature blasts in the bone marrow and the presence of ringed sideroblasts and the degree of monocytosis.
5 subgroups: refractory anemia (RA), refractory anemia with ringed sideroblasts (RARS), refractory anemia with excess blasts in transformation (RAEB-T , chronic myelomonocytic leukemia (CMML) and refractory anemia with excess blasts (RAEB).
FAB classification:
Refractory anemia-10-40% of cases, with <5% blasts. AML tranformation 10-20%.
Refractory anemia with ringed sideroblasts-10-20% of cases, <5% blasts,AML transformation 10%, >15% ringed sideroblasts.
Refractory anemia with excess blasts-25-30% cases, 5-20% blasts, 40-50% AML transformation.
Chronic myelomonocytic leukemai-10-20% cases, <20% blasts, AML transformation 20%, greater than 10 the 9th monocytes.
Refractory anemia with ringed sideroblasts in transformation-10-30% of cases, 21-30% blasts, 50-60% transformation to AML.
Refractory anemia with the ring sideroblasts generally have a benign clinical course (Malcovati L et al).
As many as 2/3 of patients with MDS have thrombocytopenia prior to treatment.
Romiplostim and eltrombopagin bind and activate the thrombopoietin receptor on megakaryocyte precursors promoting cell proliferation and have been useful in patients with severe thrombocytopenia and lower risk MDS.
Genetic abnormalities that may be seen in inherited sideroblastic anemiaa include loss of function mutations in the genes ALAS2, ABCB7, and SLC25A48, and in ring sideroblasts in myelodysplastic syndromes have up regulation of genes involved in the synthesis and down regulation of ABCB7.
Recurrent mutation of the SF3B1 gene is found in 20% of patients with myelodysplastic syndromes.
SF3B1 gene mutations are found in 65% of patients with ring sideroblastic anemias, and even among other subtypes of myelodysplastic syndromes with large numbers of ring sideroblasts in the marrow, such a gene mutation frequency is common.
Mutations in SF3B1 mutations commonly have ringed sideroblasts and a more indolent clinical course.
Myelodysplastic syndrome-WHO classification and criteria RA-anemia, no or rare blasts BM-erythroid dysplasia, <5% blasts, <15% RS
RARS-anemia, no blasts BM-erythroid dysplasia 15% or greater RS, <5% blasts.
RCMD (refractory cytopenia with multilineage dysplasia) bicytopenia to pancytopenia with no or rare blasts, no Auer rods, <1 x 109th monocytes/L BM dysplasia 10% or greater I 2 or more myeloid cell lines, <5% blasts, no Auer rods, <15% RS
RCMD-RS-bi or pancytopenia, no or rare blasts in blood, no Auer rods and <1 x 10th to 9th monocytes per liter. BM dysplasia >10% of cells in > 2 myeloid cell lines, >15% RS, <5%blasts and no Auer rods.
Patients with refractory anemia and refractory anemia with ringed sideroblasts have a low risk for progression to acute myeloid leukemia.
Clinical discrimination between the myelodysplastic syndromes and secondary AML is predominantly on cytomorphologic analysis, since patients with MDS heve dysplastic hematopoiesis and a myeloblast count of less than 20%, whereas those with a myeloblast count of 20% or more have AML.
Several genes have recurrent mutations during the evolution from the myelodysplastic syndromes to secondary AML-FLT3, NPM1, RUNX1, TP53 and NRAS.
More than 25% of cases have large numbers of ring sideroblasts in the bone marrow.
Patients with unexplained cytopenias and suspected MDS should have bone marrow examination to include a full cytogenic analysis to assess the metaphase karyotype, iron staining of an adequate aspirate to evaluate for the presence of ringed sideroblasts, a core biopsy and a peripheral blood smear for morphologic evaluation.
Ring sideroblasts usually seen on iron staining of marrow aspirate erythrocytes with a complete or partial ring of iron laden mitochondria surrounding the nucleus.
Patients with refractory anemia and refractory anemia with ringed sideroblasts have anemia as a result of ineffective erythropoiesis and high rate of erythroid apoptosis.
(International Prognostic Scoring system) defines a sum score of bone marrow blasts, karyotype and cytopenias.
Bone marrow findings include nuclear budding, bridging, megaloblastic changes and ringed siderblasts.
Dysplastic megakaryocytes include small mononuclear megakaryocytes, thr presence of discrete nuclear lobes, and granulocyte nuclear hypolobulation and decreased cytoplasmic hypogranularity.
(International Prognostic Scoring System) grouped into 4 categories, from low to high-risk based on risk factors: marrow blast percentage, number of cytopenias, and marrow blast karyotypes.
Approximately 1/2 of patients will have a normal karyotype.
Bone marrow blasts- <5% (score 0), 5-10% (score 0.5%, 11-20% (score 1.5), 21-30% (score 2.0).
Karyotype-Good (score 0), intermediate (score 0.5) and poor (score 1.0)
Cytopenias-0-1 lineage (score 0)2 or 3 lineages (score 0.5)
International Prognostic Scoring System () categories correlate with survival with median survival of 5.7 years, 3.5 years, 1.2 years and 0.4 years for patients with low, intermediate-1, intermediate-2, and high risk disease, respectively.
Aproximately two-thirds of patients have lower risk disease as defined by the and includes low-risk and intermediate-1 risk disease: associated with an indolent course and prolonged survival expectations.
Overall survival for poor cytogenetics and highest risk bone marrow blast counts (21-30%) are comparably low at 9 and 11 months, respectively.
Patients with higher risk account for 29% of patient population, 22% with Int-2 disease and 7% with h�igh risk disease.
In patients with higher risk MDS they develop AML or die from complications of the disease on average within 1 1/2 years
Approximately 25% of newly diagnosed patients and 15-20% of established patients have a higher risk of disease.
WHO Performance Scoring System in contrast to uses time dependent covariables so that risk assessment is reassessed upon progression of disease, and can be applied at anytime during a patient’s disease course.
Median survival in untreated patients with Int-2 and high risk myelodysplastic disease is 1.1 years and 0.4 years, respectively.
Median time to development following chemotherapy 4-5 years
Therapy related myelodysplasia and acute myelogenous leukemia after high-dose chemotherapy is between 5% and 15%.
Leading causes of death are bone marrow failure complications of bleeding and infection.
AML arising from myelodysplastic syndrome almost always lethal.
Infections arising in the presence of neutropenia kill 40-65% of affected patients.
In early stage disease aberrant immune attack on myeloid progenitors result in increased increased apoptosis with bone marrow failure.
Evaluation of peripheral blood smears may reveal morphologic changes such as macrocytosis, hypogranulated neutrophils with hyposegmented nuclei-pseudo-Pelger-Huet anomaly and giant platelets.
Circulating myeloblasts may be seen in advanced disease.
Secondry acute myelogenous develops in approximately one third of persons with MDS.
Associated with a number of chromosome abnormalities including: deletions of chromosome 7q, 5q, 6q, 11q, 13q, and 20q or trisomy 8.
Deletions of chromosomes 7q an 5q most common chromosomal abnormalities.
Approximately 50% of patients harbor a deletion of all or part of chromosome 5 or 7 or trisomy 8.
Chromosome 7 and multiple chromosomal abnormalities associated with poor outlook.
Isolated del5q asssociated with a better prognosis.
TNF promotes apoptosis in erythroid cells in the early stages of MDS, reflecting ineffective hematopoiesis and hypercellular bone marrow with peripheral cytopenias.
The stromal microenvironment in MDS impairs the ability to support cellular differentiation.
Some forms of MDS associated with autoimmune diseases and in some patients treated with immunosuppresive agents responses can occur.
Aim of treatment for lower risk patients is for hematologic improvement and for higher risk patients the aim is to alter the natural history of the disease.
Management is complicated by the advanced age of patients, the presence of non-hematological comorbidities and relative inability to tolerate intensive forms of therapy.
When the illness progresses into AML, there is a lower response rates to standard therapy than those with denovo AML.
Not all patients are treated immediately, and in patients with mild cytopenia surveillance is the best approach.
The administration of erythropoiesis stimulating agents can ameliorate anemia in patients with low risk MDS and is the first therapeutic option for most of such patients with anemia.
A serum EPO level below 200 milliunits per milliliter is the most reliable predictor of a response, whereas a high transfusion requirement predicts treatment failure.
ESA‘s have a median duration of a response in the order of one to two years.
Secondary to chemotherapy or radiation has a more unfavorable clinical course and higher rate of progression to acute myelogenous leukemia than does primary myelodysplastic syndrome.
Allogeneic stem cell transplantation only curative treatment at this time.
Allogeneic hematopoietic stem cell transplantation is considered curative treatment for younger patients with MDS.
Older patients with MDS undergoing hematopoetic stem cell transplant have similar overall survival compared with younger patients.
The use of younger matched unrelated donors is associated with significant lower relapse rate and higher disease-free survival compared with allogeneic hematopoietic cell transplant using older matched sibling donors.
Reduce intensity or non-myeloablative conditioning regimens has resulted in substantial reduction and transplant related toxicity and mortality.
Disease-free survival rates following allogeneic hamatopoietic cells transplant is between 29 and 40%.
Cure rates with allogeneic stem cell transplant 20-40%.
One study revealed a 5-year disease free survival rates of 60%, 36%, and 28% after bone marrow transplant in low, intermediate and high risk disease groups.
Treatment related mortality with allogeneic stem cell transplants in such patients as high as 43%.
The number of blast cells present and not being in complete remission at the time of hematopoietic stem cell transplantation are the most significant factors leading to inferior outcomes.
Generally agreed that allogeneic hematopoietic stem cell transplant should be offered to patients with intermediate two-or high risk disease according to IPS as criteria.
Dose-reduced conditioning followed by allogeneic stem-cell transplant for myelodysplastic syndrome results in at least an equivalent survival trend for a better 2-year overall survival, especially in cytogenetic low-risk group and is an alternative to a myeloblative regimen, and should be considered in older patients.
Presently, 4 drugs are approved for MDS: azacitidine, lenalidomide, decitabine and Ivosidenib.
These agents can improve hematopoiesis, delay disease progression, and improve survival for a subset of patients: however only a few patients with MDS respond and benefit is temporary.
Allogeneic hematopoetic stem cell transplant is the only potential curable therapy, but owing to advanced age of patients and frequency of comorbid conditions, less than 10% of patients can undergo stem cell transplant.
MDS sensitive to 5-azacytidine and decitabine drugs that reverse DNA methylation.
Response rates with low-dose cytosine arabinoside 15-20%.
Immunosuppressive drugs may be useful in patients who experience T cell mediated suppression of hematopoiesis.
Antithymocyte globulin and cyclosporin A may be useful in low-risk patients with refractory anemia.
30% response rate for Valproic in elderly patients with refractory anemia and excess blasts with unfavorable features, and it may particularly help thrombocytopenia.
Hypomethylating agents 5-azacitidine and decitabine delay transformation to acute myeloid leukemia.
Hypomethylating agents are administered at one tenth tolerable doses suggesting that azacitidine and decytabine work at lower doses in a different way than they do at higher doses: at higher doses they are cytotoxic agents, at lower doses they are hypomethylating agents.
Hypomethylating agents at lower doses do not initiate events that kill cells, but alter signaling in the cell by a re-expressing genes that are apparently silenced.
Hypomethylating agents can turn off promoter hypermethylation which can turn off suppressor genes that control growth and differentiation of cells or regulation of other genes: these agents can reverse the abnormal process and re-express the gene
Azacitidine in 358 patients with advanced disease compared to conventional care resulted in a median survival of 24.4 months vs. 15 months for conventional care regimens (Juliusson G), and analysis indicated the drug was favored despite age, gender, score, cytogenetics, subtype of disease or LDH levels.
Azacitidine 75 mg/m2/day for 7 days of a 28 day cycle plus placebo or subcutaneous romiplostim 500 mg or 750mg per week on a randomized basis: incidence of thrombocytopenia events per cycle higher in placebo group (85%) than in the Romiplostim 500 mg (69%) and 750 mg (64%) groups, also 69% of placebo group received platelets, in comparison to 46% and 36% for the romiplostim 500 mg and 750 mg, respectively (Kantarijian ).
Azacitidine and Lenalidomide combination therapy is well tolerated and highly active in patients with high-risk MDS: a phase II study involving 36 patients with high-risk MDS who received azacitidine (75 mg/m2 daily for 5 days) and lenalidomide (10 mg daily for 21 days) in seven 28-day cycles.-overall response rate was 72%, and the complete response (CR) rate was 44% (Sekeres MA et al).
In the above study hematological improvement was observed in all cell lines, and median time to response was 3.7 months with a median duration of CR was 17+ months and a median overall survival (OS) was 13.6 months, and median OS among those with CR was 37+ months.
Azacitidine increased survival by 74% in patients treated with intermediate 2 to high risk for myelodysplasia compared to three conventional treatments (Fenaux).
Transfusional hemosiderosis infrequently encountered because median age at diagnosis is advanced and survival less than 5 years.
Presently, no study has demonstrated an association of attainment of complete remission with extended survival (Cheson BD, 2009).
Patients with iron overload have higher mortality rates due to liver and cardiac abnormalities.
The seriously of an MDS diagnosis is determined by the Revised International Prognostic Scoring System (IPSS -R) or the IPS molecular (IPSS-M) systems.
Both systems incorporate numbers, and degrees of cytopenia, karyotype abnormalities, and myeloblast percentage in the bone marrow or blood at diagnosis that are used to generate a score that accurately predicts survival and AML transformation rates.
The IPSS-M includes information on 31 Gene mutations to define the accuracy the IPSS-R.
In a study of 178 patients with low or intermediate-1 International Prognostic Scoring System (IPSS) scores the median survival for patients receiving iron chelation therapy was not reached at 160 months compared to those not receiving such therapy at 40.1 months, indicating that controlling transfusions and adding an iron chelation rate improves symptoms and overall survival.
Erythropoietin one of the most common used growth factors for treatment.
The most frequent therapy for moderate to advanced anemia is the off-label use of erythropoiesis stimlating agents.
Patient whose MDS include ring and/or an SF3B1 mutation may benefit from luspatercept, which promotes late stages of erythropoiesis.
The pateints most likely to benefit from ESAs have a pretreatment serum erythropoietin livel of less than 100 U/L, IPSS low-risk and a low number of required transfusions.
In low-risk patients with EPO levels above 200-500 U/L and in patients harboring del(5q) and are transfusion dependent, alternatives to EPO therapy such as lenalidomide should be considered: can result in transfusion independence in approximately 3 of 4 patients.
A EPO level of greater than 500 U/L associated with a very low likelihood of benefiting from EPO treatments.
Erythropoietin useful in patients with low serum erythropoietin levels <500 U/ml, with minimal red blood cell transfusion requirement <2/ month and a bone marrow with fewer than 10% blasts.
For patients with significant transfusion requirement erythropoietin has a response rate of 10%.
Prophylactic dosing of G-CSF does not have any effect on MDS progression or infection risk.
Thrombopoietin agonsits nomiplostin and eltrombopag can modestly reduce platelet transfusion needs, and modestly reduce clinically signficant bleeding episodes.
There are three drugs approved for myelodysplastic syndrome they include azacitidine, decitabine and lenalidomide.
Azacitidine is the only drug shown in randomized, perspective, phase 3 trials to prolong survival in patients with high risk MDS compared with conventional care, regiments, low-dose, chemotherapy or AML therapy.
Lenalidomide induces transfusion independence in about 2/3 patients with low risk MDS and isolated del(5q), and many patients with a response have a cytogenetic remission, clearly indicating that it is a true targeted therapy.
After 2 to 3 years most patients have a re-emergence of the del (5q) clone and recurrence of anemia.
Relapse is caused by a selection of hematopoetic cells resistance to resistant to Lenalidomide and frequently carry a somatic mutation of TP53 or RUNX 1, which is typically drives leukemic transformation.
These agents can improve hematopoiesis, delay disease progression, and improve survival for a subset of patients: however only a few patients with MDS respond and benefit is temporary.
Allogeneic hematopoetic stem cell transplant is the only potential curable therapy, but owing to advanced age of patients and frequency of comorbid conditions, less than 10% of patients can undergo stem cell transplant.
In a phase three study of patients with high risk disease Azacitidine treated patients had an overall survival of 24.4 months compared to 15 months for patients treated with conventional management and a 51% response rate versus a 26% response rate, respectively.
Phase I study of patients with high risk MDS treated with combination of Azacitidine 75mg/m2 subcutaneous days 1-5 plus lenalidomide 10 mg orally days 1-21 resulted in a 71% response rate among 17 evaluable patients with 7 complete responses and 1 partial response and 3 with hematologic improvement and 11 marrow complete remission (Sekeres).
Lenalidomide may work by blocking the effect of cytokines that cause premature death of cells in the bone marrow and by its direct action on 5Q deletion cytogenetic changes in some patients.
Thalidomide and lenalidomide inhibit angiogenesis and tumor necrosis factor and the former associated with an almost 20% rate of RBC transfusion independence or a greater than 50% decrease in required transfusions.
A combination of azacitidine and lenalidomide in high-risk patients showed an overall response rate of 67% (azacitidine 75 mg/m2 daily for five days
10 mg daily for 21 days) (Cleveland Clinic).
In a phase II trial evaluating Clofarabine in 36 patients revealed a complete remission rate 29% and 25% of patients, in intravenous and oral administered drug, respectively (Faderl S).
Promising new agents include luspatercept, Rigosertib, , IDH inhibitors, small molecules targeting apoptosis, and guadecitabine.
The FDA has approved an oral combination comprised of decitabine and cedazuridine for the treatment of select adult patients with myelodysplastic syndromes.
The combination is indicated for patients with previously treated and untreated, de novo and secondary MDS with the following subtypes: refractory anemia, refractory anemia with ringed sideroblasts, refractory anemia with excess blasts, and chronic myelomonocytic leukemia (CMML).
The regimen is also indicated for patients with intermediate-1, intermediate-2, and high-risk International Prognostic Scoring System groups.
Trial ASTX727-01-B enrolled a total of 80 adult patients with MDS who were classified via the International Prognostic Scoring System as intermediate-1, intermediate-2, or high-risk or CMML.
Trial ASTX727-02 (NCT03306264) included 133 adult patients with MDS or CMML, including all French-American-British classification criteria and IPSS intermediate-1, intermediate-2, or high-risk prognostic scores.
In both trials, patients were randomized 1:1 to receive either 35 mg decitabine and 100 mg cedazuridine orally in cycle 1 and decitabine 20 mg/m2 intravenously in cycle 2 or the reverse sequence.
Luspatercept is a modified activin receptor IIB-IgG Fc fusion protein that targets transforming growth factor beta (TGF-B) signaling and differentiation factor 11 enhancing late-stage red blood cell (RBC) maturation.
In patients with lower risk MDS; luspatercept was developed for transfusion-dependent, anemic patients who do not meet criteria for erythropoiesis stimulating agents (ESA) therapy or who have failed to respond to such treatment.
Luspatercept has shown the most promise for patients with ringed sideroblasts (RS), particularly those harboring mutant SF3B1.
Luspatercept is a Recombinant fusion protein that binds transforming growth factor beta super family ligands to enhance late stage erythropoiesis.
In patients with ring sideroblasts luspatercept results in transfusion independence in 38 cases 38% of cases.
In a phase 2 trial, 63% of the 51 patients treated with higher-dose luspatercept achieved hematological improvement-erythroid, and 38% of 42 patients eligible for RBC transfusion independence (RBC-TI) achieved RBC-TI.
Luspatetcept approved for the Treatment of transfusion dependent MDS and ring sideroblasts who have not had a response to erythropoiesis stimulating agents.
The PACE-MDS study also revealed a significant response among patients with ringed sideroblast levels of at least 15% and SF3B1 mutations; 69% and 77% achieved hematological improvement, respectively.
A phase 3 trial (MEDALIST) enrolled participants with lower risk MDS with RS with the primary endpoint of RBC-transfusion independence for at least 8 weeks: luspatercept 1 mg/kg subcutaneously every 21 days or placebo in a 2:1 randomized fashion.
Some patients with hypoplastic MDS, transfusion independence can be achieved with immunosuppressive therapy, particularly with anti-thymocyte globulin combined with cyclosporine.
Of the patients who received luspatercept 38% met the primary endpoint of RBC-TI compared with 10 participants (13%) in the placebo group with a mean hemoglobin of >1.5g/dL for 8 weeks.
Luspatercept treatment-related adverse events (AEs) included fatigue, dizziness, asthenia, and diarrhea.
Imetelstat is a telomerase inhibitor for lower risk MDS patients who are transfusion-dependent and have failed with ESA.
It has achieved complete responses in the setting of U2AF1 or SF3B1mutations of myelofibrosis.
Iron chelation therapy is a key component of managing lower risk MDS patients with transfusion requirement.
TELESTO trial evaluated the safety and efficacy of deferasirox vs placebo in 225 adults diagnosed with low/intermediate-1 MDS who had iron overload: Patients in the deferasirox group experienced significantly longer median event-free survival compared with the placebo group; 1440 days vs 1091 days
The median overall survival (OS) was not significantly different between the two groups.
Combining histone deacetylase inhibitors with hypomethylating therapy thus far has not yielded significant improvements in MDS treatments.
The use of hypomethylene agent is azacitidine or decitabine, currently represent the most common initial treatment in patients with higher risk MDS who are an eligible for transplantation.
About half of patients with azacitidine have a hematological response.
Treatment is associated with prolonged survival in the order of a few months.
For patients with high-grade MDS, DNA methyltransferase inhibitors such as azacitidine and DAC are standard therapies, unless they undergo an allo-HCT.
Unfortunately, some patients show no response to DNA methyltransferase inhibitors, while many relapse after achieving an initial response.
Mutations commonly seen in MDS include those of SF3B1, SRSF2 and U2AF1.
The mutations result in dysregulated mRNA splicing, which leads to myelodysplasia.
Isocitrate dehydrogenase 2 (IDH2) mutations are present in approximately 5% of patients with MDS.
IDH2 mutations are associated with DNA and histone hypermethylation, altered gene expression, and impaired differentiation of hematopoietic progenitor cells.
Hypomethylating agents may increase the expression of programmed death 1 (PD-1), programmed death ligand 1 and cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) in MDS CD34+ cells.
Deregulation of BCL-2 family proteins have been identified in bone arrows of MDS patients.
BCL-2 overexpression in higher risk MDS, may cause antiapoptotic resistance.
BCL-2 blockade by venetoclax in high-risk AML patients have had encouraging results.
Ivosidenib approved for MDS with IDH1 mutation.