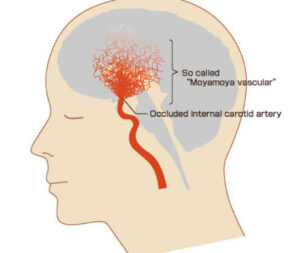
A progressive occlusive disease of the cerebral vasculature with particular involvement of the circle of Willis and the arteries that feed it.
A non-inflammatory, non-atherosclerotic cerebrovascular disorder, characterized by progressive stenosis of the terminal internal carotid artery, leading to fragile collateral vessel?l9 formation.
Moyamoya disease occurs in 0.1 per 100,000 people worldwide, but the prevalence is substantially higher in East Asia, especially Japan (17.6 per100,000).
Moyamoya disease, approximately twofold more common among females than males and has a mortal distribution at 10 years and at 30 to 50 years.
A family history reported in 12 to 15% of patients with the disease.
Underlying pathophysiology is unknown, but may involve alterations in genes involving vascular development and angiogenesis: MMP, VEGF, and PDGFRB.
The RNF 213 P.R4 810 K gene variant increases the risk of Moyamoya disease among Asian patients.
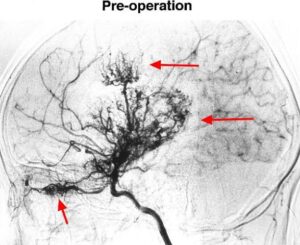
Diagnosis is made on basis of digital subtraction and angiographic findings with stenosis or occlusion of anterior arteries in the terminal portion of the intracranial internal carotid artery and abnormal vascular networks in the vicinity of the stenotic lesions.
Brain MRI or MRA are less accurate with diagnosis, particularly in patients with unilateral lesions for those older than 60 years or in early stage disease.
Angiographic changes of vascular collateral networks that develop adjacent to stenotic vessels.
Stenotic occlusive blood vessels usually bilateral.
Characterized by intimal thickening in the walls of the terminal portions of the internal carotid vessels bilaterally.
Consists of nonarteriosclerotic narrowing of the distal internal carotid arteries in the proximal branches.
Proliferating intima may contain lipid deposits, with thinning of the media.
The anterior, middle, and posterior cerebral arteries that emanate from the circle of Willis may show varying degrees of stenosis or occlusion.
On angiogram these changes appear like “puff of smoke“
When these vascular abnormalities occur, typically with Down syndrome, neurofibromatosis type I, and sickle cell disease, they are classified as Moyamoya syndrome.
When the process occurs in isolation diagnosis is Moyamoya disease.
Because of decreased blood flow collateral blood vessels form.
Can occur following brain radiation, or with renal artery stenosis or hyperthyroidism.
Numerous small vascular channels can be seen around the circle of Willis.
Occurs more frequently in Asians than Caucasians, but have been documented in all races.
Etiology unknown.
Familial 10% of the time, suggesting familial relationship and autosomal dominance with reduce penetrance.
Patients usually present with ischemic strokes .
Some individuals present with hemorrhagic stroke, headaches, or other neurological changes.
Diagnostic confirmation occurs with MRI or angiography.
May be associated with autoimmune disease-up to 22% disease.
Type I diabetes, thyroiditis and hyperthyroidism are more prevalent.
CSF abnormal in 80-90% of cases, usually with an increase in leukocytes and increase total protein.
Needs to be differentiated from CNS vasculitis, as vasculitis usual treatment is steroids or immunosuppressive agents and moyamoya is not treated with such drugs.
Moyamoya disease treatment involves managing symptoms, improving blood flow to the brain and controlling seizures.
Anticoagulants can help avoid clots and blockages, but can also increase the risk of bleeding.
In some cases, revascularization can help with surgery to rebuild the blood supply to the underside of the brain.
Surgical revascularization with a direct bypass or indirect bypass is associated with decrease risk of ischemic stroke and death.
Patients receiving non-surgical management of ischemic events have recurrent annual stroke rate of 20 to 50%.
Asymptomatic patients have 1.4% to 15% annual risk of stroke:for these patients bypass surgery is associated with a 26% reduction in the risk of death but is 76% increase in the risk of hemorrhagic events compared with non-surgical management
Limited evidence that anti-platelet therapy can be considered to Moyamoya disease.
Emdovascular treatment is associated with restenodid rates of almost 70% and high rates (9.5%) of complications of vessel rupture and intracerebral hemorrhage.