
 Subset of diffuse large B cell lymphoma with predominant mediastinal involvement, with clear cytoplasmic cells, with convoluted or centroblastic nuclei and thin bands of sclerosis.
Subset of diffuse large B cell lymphoma with predominant mediastinal involvement, with clear cytoplasmic cells, with convoluted or centroblastic nuclei and thin bands of sclerosis.
Primary mediastinal B cell lymphoma is a rare, but aggressive, mature B cell lymphoma arising from thymic B cells.
Represents 2 to 4% of non-Hodgkin’s lymphoma with a predominant among females.
Expresses B cell surface antigens CD20 and CD79a and IgH rearrangement and mutations.
CD 30 and CD 23 o are expressed in 77% and 67%, respectively, of childhood cases of primary mediastinal B cell lymphoma.
Expression of CD30 is more common in primary mediastinal large B-cell lymphoma than in other types of large B-cell lymphoma.
Like Hodgkin’s disease, it has a peak incidence in adolescents and young adults, presenting as a mediastinal mass, alterations in nuclear factor-kB and JAK/STAT signaling, and up regulation of PD-L1..
It is an aggressive C-cell lymphoma and its molecular signature is more like Hodgkin’s lymphoma rather than DLBCL (diffuse large B-cell lymphoma), and is characterized by activation of NFkB and JAK-STAT pathways and program death ligand 1 and 2 overexpression.
At the molecular level, alterations in Janus/signal transducers and activators of JAK-STAT transcription pathways.
Often has copy number alterations and rearrangements of 9p24.1.
Cells usually do not have surface IgG.
PD-1 expression in 70% of patients.
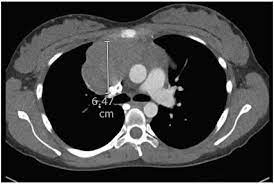
Typically presents with bulky mediastinal disease and can be associated with pleural and pericardial effusions.
It is a highly aggressive tumor, with a rapid growing mediastinal mass, usually bulky, which frequently causes a superior vena cava syndrome, other compressive symptoms, and pleural and pericardial effusions.
Most patients are diagnosed with early disease.
Rarely it is more extensive at the time of diagnosis involving extranodal sites such as the kidneys, adrenals, stomach, and ovary.
It usually does not involve the bone marrow or CNS initially.
Involvement of extranodal sites or the CNS is more frequent at the time of relapse/progressive disease.
Patients are often young and female.
Patients typically present with symptoms related to mediastinal bulky masses, which involve the chest wall, lung, pleura or pericardium.
Many patients have associated plural of pericardial effusions.
Bone marrow or CNS involvement are uncommon initially, and elevated levels of LDH and overt B symptoms can occur.
Diagnosis is a preferred excisional biopsy, but this is often not feasible, because of the respiratory and cardiac compromise.
A needle image guided percutaneous biopsy is appropriate.
Disease staging includes bone marrow aspiration, bone marrow biopsy, lumbar puncture, PET/CT scans and rapid initiation of therapy.
Approximately 20% ofpatients present with stage 3 or 4 disease.
Metastatic disease can involve the kidneys and adrenal glands.
Prognosis is good, with approximately 90% of patients cured with modern therapy.
Prognosis indicated by the International Prognostic Index (IPI), with high IPI patients having a worse prognosis than low IPI patients.
Biopsy is required for diagnosis, to rule our other types of lymphoma.
Clinically may be associated with a superior vena cava syndrome and pleural effusions.
In symptomatic patients treatment needs to start quickly.
Treatment:
First-Line Therapy
Dose-adjusted EPOCH + rituximab (DA-EPOCH-R) × 6 cycles
Preferred Regimen: DA-EPOCH-R (Dose-Adjusted Etoposide, Prednisone, Vincristine, Cyclophosphamide, Doxorubicin + Rituximab)
R-CHOP-14 × 4–6 cycles
CHOP-21 × 6 cycles
An alternative consolidation approach includes R-CHOP-14 × 4 cycles followed by ICE × 3 cycles ± rituximab (category 2B).
Currently the most widely used regimen in the US, especially at major centers
Associated with high cure rates (~90% EFS in some series) and may eliminate the need for consolidative radiation
After completion of first-line therapy, restaging with PET/CT is essential:
Complete response (PET negative, 5-PS 1–3): Active surveillance, or involved-site radiation therapy (ISRT) depending on the regimen used
Partial response (PET positive, 5-PS 4): Repeat biopsy is recommended.
Notably, persistent PET-positive masses after DA-EPOCH-R with 5-PS 4 and minimal uptake above liver on visual inspection can be observed without biopsy.
No response or progressive disease (PET positive, 5-PS 5): Repeat biopsy, then proceed to relapsed/refractory therapy
Residual mediastinal masses are common after treatment. Biopsy of a PET-positive mass is recommended if additional systemic treatment is contemplated.
For relapsed or refractory PMBCL the following options are available:
Pembrolizumab
Nivolumab ± brentuximab vedotin (category 2B; responses have been seen even with low-level CD30 positivity)
Manage as relapsed/refractory DLBCL which includes salvage chemoimmunotherapy, CAR T-cell therapy with axicabtagene ciloleucel or lisocabtagene maraleucel, and bispecific antibodies such as epcoritamab and glofitamab.
For pediatric and adolescent/young adult patients, guidelines list clinical trial enrollment as preferred, with the following suggested regimens:
DA-EPOCH-R (preferred) × 6 cycles
CHOP + rituximab × 6 cycles ± RT (avoidance of RT is strongly preferred in pediatric patients)
LMB-modified B/C chemotherapy + rituximab
For relapsed/refractory pediatric PMBCL, options include R-DHAP, R-ICE, nivolumab, pembrolizumab, brentuximab vedotin + nivolumab, and CAR T-cell therapy (axicabtagene ciloleucel or lisocabtagene maraleucel after ≥2 prior chemoimmunotherapy regimens).
DA-EPOCH-R obviated the need for radiotherapy in the vast majority of patients, with a 93% event-free survival and 97% overall survival at a median follow-up of 5 years.
(DA-EPOCH-R Rituximab (an immunotherapy)Etoposide (chemotherapy)Prednisone (a steroid)Oncovin (the brand name for Vincristine, chemotherapy)Cyclophosphamide (chemotherapy)Hydroxydaunorubicin (also known as Doxorubicin, chemotherapy)
A study of 157 patients found comparable efficacy between R-CHOP ± RT and DA-EPOCH-R ± RT, with similar CR rates (~75–77%) and no significant differences in PFS or OS.
However, DA-EPOCH-R was associated with significantly higher toxicity (29.9% vs. 16.2%)
A PET-adapted approach using R-CHOP has also shown favorable outcomes, with a 5-year time to progression of 80% and OS of 89%, and the use of end-of-treatment PET to guide consolidative RT reduced the need for radiation in the majority of patients.
Generally followed by consolidative mediastinal radiation (30–36 Gy).
The trend in PMBCL management is toward a PET-guided approach to consolidative RT.
Patients achieving a complete metabolic response (Deauville 1–3) after chemoimmunotherapy may safely omit RT, while those with residual PET positivity require biopsy confirmation before proceeding with additional therapy.
This is particularly important given the young age of most PMBCL patients and the long-term risks of mediastinal RT (cardiac toxicity, secondary malignancies, breast cancer).
Radiation carries long-term risks: breast cancer, coronary artery disease, lung toxicity — especially relevant in young women.
PMBCL is characterized by frequent 9p24.1 amplification leading to PD-L1/PD-L2 overexpression, providing a strong biological rationale for PD-1 inhibitor therapy.
Both pembrolizumab (FDA-approved for relapsed/refractory PMBCL) and nivolumab have demonstrated meaningful activity in this setting.
CAR T-cell therapy also shows promise, with analysis suggesting that prior checkpoint inhibitor exposure may enhance anti-tumor efficacy of subsequent CAR T-cell therapy, though with a potential increase in non-relapse mortality.
Interim PET/CT (after 2–4 cycles) guides dose adjustment in DA-EPOCH-R
End-of-treatment PET/CT is critical
Deauville score 1–3: Complete metabolic response → surveillance Deauville 4–5: Residual disease → biopsy to confirm viability before escalation
Residual mediastinal masses are common and do not always represent active disease — PET-guided biopsy is essential before declaring refractory disease.
Relapsed / Refractory Disease
2nd Line (Bridge to transplant or CAR-T):
R-ICE, R-DHAP, R-GDP (platinum-based salvage) Response rates lower than other DLBCLs
Pembrolizumab (anti-PD-1): Highly active in R/R PMBCL; FDA-approved. PMBCL overexpresses PD-L1/PD-L2 due to 9p24.1 amplification — this is a biologic vulnerability
Nivolumab: Also active
CAR-T cell therapy (axicabtagene ciloleucel, lisocabtagene maraleucel): Options in multiply relapsed/refractory disease
Consolidation in responders:
Autologous stem cell transplant (ASCT) remains standard for chemosensitive relapsed disease
Key Biologic Features Relevant to Therapy
CD20+ → rituximab backbone essential
9p24.1 amplification → PD-L1/PD-L2 overexpression → checkpoint inhibitor sensitivity
JAK-STAT pathway activation (JAK2 amplified at 9p24.1)
Shares molecular features with classical Hodgkin lymphoma
Prognosis
Cure rates with modern therapy: ~85–90% in first-line
Prognosis in truly refractory disease is poor but improving with immunotherapy and CAR-T
Traditionally treated with CHOP or combination chemotherapy with eoposide, leucovorin, doxorubicin, cyclophosphamide, vincristine, prednisone and bleomycin, followed by radiotherapy.
To avoid radiotherapy newer approaches with rituximab, etoposide, doxorubicin, cyclophosphamide, vincristine and prednisone alone have been highly successful.
Treatment with rituximab, cyclophosphamide, doxorubicin vincristine and prednisone followed by radiation produces cure rate between 75 and 80% and long-term survival of 85-90%.
For patients with primary mediastinal B-cell lymphoma (PMBCL) who achieved a complete metabolic response after immunochemotherapy, radiation therapy may be safely omitted without heightening their risks of relapse or disease progression – thereby sparing them the toxicity and costs of this additional treatment.
Recurrent or refractory patients have a poor prognosis.
Checkpoint inhibitors associted with good responses for refractory patients.
Primary B cell mediastinal lymphoma is radiosensitive, however, its role is not clear given the effectiveness of intensive chemotherapy.
The role of PET/CT scans in evaluating end of treatment plans has not yet been clarified.
Circulating tumor, DNA (ctDNA) is a potential biomarker for the diagnosis, prognosis, response, assessment, and remission monitoring.
Most patients who do not experience a response to initial treatment will experience will disease progression.
Recurrent disease commonly occurs within eight months of the initiation of therapy and with more than half of progressions occurring in less than one year.
Sites of relapse, including the mediastinum with new or extranodal disease, the lung liver, kidney, and adrenal glands.
CNS disease is rare at initial presentation, but may occur later in the disease.
Refractory and relapse patients require additional aggressive combination chemotherapy followed by consolidation with high-dose chemotherapy and autologous stem cell transplant that can result in an overall survival rate of 65 to 68%.
Checkpoint inhibitors, BTK inhibitors, and anti-CD 19 CAR T cell therapy are being investigated for relapse and refractory disease.