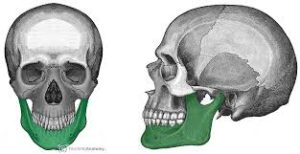
The mandible, lower jaw or jawbone is the largest, strongest and lowest bone in the human facial skeleton.
The mandible forms the lower jaw and holds the lower teeth in place.
it assists in mastication and forms the lower jawline.
The the jawbone, is the largest and strongest bone in the human skull.
It is a vital component of the facial structure and plays crucial roles in functions such as chewing, speaking, and facial expression.
The mandible is a U-shaped bone that forms the lower jaw.
It consists of a horizontal body and two vertical branches called rami. The rami come together at the midline, forming the mandibular angle or chin.
The mandible articulates with the temporal bone at the temporomandibular joints (TMJ).
These joints allow the jaw to open and close, as well as move sideways and forward for actions like chewing, talking, and yawning.
The lower set of teeth, known as the mandibular dentition, is anchored within the alveolar processes of the mandible.
The mandibular teeth work together with the upper teeth to facilitate chewing and the breakdown of food.
Various muscles attach to the mandible, enabling movement and providing stability.
Muscles involved include the muscles of mastication, such as the masseter, temporalis, and medial pterygoid muscles.
The mandible contributes to the overall facial appearance and symmetry.
The shape and position of the mandible can impact the profile and contours of the lower face and chin.
The mandible acts as a protective barrier for the lower part of the face, including the tongue, salivary glands, and parts of the throat.
It helps safeguard these structures from external forces and trauma.
7Like other bones in the body, the mandible undergoes ossification to develop and grow.
It starts as two separate bones that eventually fuse together during early childhood.
The mandible is commonly used for dental implant procedures, where artificial tooth roots are surgically placed into the bone to support replacement teeth.
The strong nature of the mandible provides a stable foundation for dental restorations.
The mandible can be affected by various conditions, including fractures, tumors, infections, and temporomandibular joint disorders (TMD).
These conditions can affect the function and aesthetics of the jaw and may require medical or dental intervention.
It sits beneath the maxilla, and is the only movable bone of the skull, except for the ossicles of the middle ear.
The mandible is composed of the body and the ramus and is located inferior to the maxilla.
The mandible is connected to the temporal bones by the temporomandibular joints.
The mandible consists of:
The body, at the front
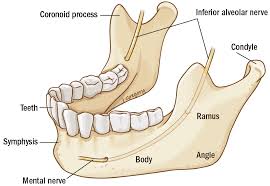
A ramus on the left and the right, the rami rise up from the body of the mandible and meet with the body at the angle of the mandible or the gonial angle.
The body is a horizontally curved portion that creates the lower jawline.
The mandible front part gives structure to the chin.
It has two surfaces and two borders.
The mandible is marked in the midline by a faint ridge, indicating the mandibular symphysis, the junction of the two halves of the mandible.
This ridge divides below and encloses a triangular eminence, the chin.
The base of the chin is depressed in the center but raised on both sides to form the mental tubercle.
The mentalis muscles attach to a depression called the incisive fossa.
Below the second premolar tooth, on both sides, midway between the upper and lower borders of the body, are the mental foramen, for the passage of the mental vessels and nerve.
Upward from each mental tubercle is the oblique line, which is continuous with the anterior border of the ramus.
Attached to this is the masseter muscle, the depressor labii inferioris and depressor anguli oris, and the platysma.
The mandible is composed of the body and the ramus and is located inferior to the maxilla.
The rami are two vertical processes located on either side of the body; they join the body at the angle of the mandible.
At the superior aspect of each ramus, the coronoid and condylar processes articulate with the temporal bone to create the temporomandibular joint which permits mobility.
Other than the ossicles of the ear, the mandible is the only skull bone that is mobile, allowing the bone to contribute to mastication.
At birth, the mandibular symphysis is composed of fibrocartilage, but within one year of life, the symphysis fuses and a subtle ridge remains at midline on the anterior surface of the body.
The body of the mandible is the anterior portion of the mandible and is bound by two surfaces and two borders.
The body ends and the rami begin on either side at the angle of the mandible, also known as the gonial angle.
The external surface contains the mandibular symphysis at midline, detected as a subtle ridge in the adult.
The inferior portion of the ridge divides and encloses a midline depression called the mental protuberance.
The edges of the mental protuberance form the mental tubercle.
Laterally to the ridge is a depression known as the incisive fossa.
Below the second premolar is the mental foramen, in which the mental nerve and vessels exit.
The alveolar border, which is the superior border, contains the hollow cavities in which the lower sixteen teeth reside.
The inferior border of the mandible creates the lower jawline and contains a small groove in which the facial artery passes.
The ramus contributes to the lateral portion of the mandible on either side.
The coronoid process and condyloid process are located at the superior aspect of the ramus.
The coronoid process is anterior and the condyloid process is posterior, and they the two are separated by the mandibular notch.
Lateral surface: provides the origin for the masseter muscle.
Medial surface: The medial surface contains the mandibular foramen through which the inferior alveolar nerve and inferior alveolar artery enter and subsequent course the mandibular canal.
Superior border: The superior border which gives rise to the coronoid and condyloid processes.
Inferior border: The inferior border is continuous with the inferior border of the mandibular body and contributes to the jawline.
Posterior border: The posterior border is continuous with the inferior border of the ramus and is deep to the parotid gland.
The coronoid process is located at the superior aspect of the ramus.
The temporalis muscle and masseter insert on its lateral surface.
The condyloid process is also located at the superior aspect of the ramus and is divided into two parts, the neck and the condyle.
The condyle contributes to the temporomandibular junction by articulating with the articular disk.
The mandible is the second bone to ossify, following the clavicle.
The first pharyngeal arch, known as the mandibular arch, gives rise to the Meckel cartilage. This cartilage serves as a template for the development of the mandible. A fibrous membrane covers the left and right Meckel cartilage at their ventral ends, each of which gives rise to a single ossification center. These two halves eventually fuse via fibrocartilage at the mandibular symphysis. Thus,
At birth, the mandible is still composed of two separate bones.
Ossification and fusion of the mandibular symphysis occurs during the first year of life, resulting in a single bone.
The mandible changes throughout an individual’s life.
Blood supply to the mandible is from small periosteal and endosteal vessels.
The periosteal vessels arise mainly from the inferior alveolar artery.
The periosteal vessels supply blood to the ramus of the mandible.
The endosteal vessels arise from the peri-mandibular branches of the maxillary artery, facial artery, external carotid artery, and superficial temporal artery.
The endosteal vessels supply the body of the mandible.
The mandibular teeth are supplied by dental branches from the inferior alveolar artery.
Lymphatic drainage of the mandible and mandibular teeth are primarily from the submandibular lymph nodes.
The mandibular symphysis region drains into the submental lymph node, which subsequently drains into the submandibular nodes.
The primary nerve associated with the mandible is the inferior alveolar nerve, which is a branch of the mandibular division of the trigeminal nerve.
The inferior alveolar nerve enters the mandibular foramen and courses anteriorly in the mandibular canal where it sends branches to the lower teeth and provides sensation.
At the mental foramen, the inferior alveolar nerve branches into the incisive and mental nerve.
The mental nerve exits the mental foramen and courses superiorly to provide sensation to the lower lip.
The incisive nerve runs in the incisive canal and provides innervation to the mandibular premolar, canine, and lateral and central incisors.
Muscles of the mandible:
Mentalis – originates from the incisive fossa
Orbicularis oris – originates from the incisive fossa
Depressor labii inferioris – originates from the oblique line
Depressor anguli oris – originates from the oblique line
Buccinator – originates from the alveolar process
Digastric anterior belly – originates from the digastric fossa
Mylohyoid – originates from the mylohyoid line
Geniohyoid – originates from the inferior portion of the mental spine
Genioglossus – originates from the superior portion of the mental spine
Superior pharyngeal constrictor – originates partially from the pterygomandibular raphe, which originates from the mylohyoid line
Muscles Inserting on the Mandible
Platysma – inserts on the inferior border of the mandible
Superficial masseter – inserts on the lateral surface of the ramus and angle of the mandible
Deep masseter – inserts on the lateral surface of the ramus and angle of the mandible
Medial pterygoid – inserts on the medial surface of the mandibular angle and ramus of the mandible
Inferior head of the lateral pterygoid – inserts on the condyloid process
Temporalis – inserts on the coronoid process
Males generally have squarer, more prominent mandibles than females, due to the larger size of the mental protuberance in males and the decreased gonial angle.
The gonial angle is 90 degrees in males, compared to 110 in females.
A cleft chin can result from inadequate or absent fusion of the mandibular symphysis during embryonic development,
often resulting in a depression of the overlying soft tissue at the midline of the mandible.
A cleft chin is a genetic condition that is inherited in an autosomal dominant fashion and found more frequently in the male population.
Orthognathic surgery includes: mandible osteotomies and sagittal split osteotomies to improve bite malalignment, sleep apnea, temporomandibular joint disorders, and structural issues such as cleft palate and micrognathia.
Mandible osteotomy is performed on patients with micrognathia, a condition in which the mandible is undersized.
Micrognathia may result in pain and difficulty chewing: correction is often needed: transecting the mandible between the first and second molars, bilaterally; the mandible is extended into its new position and stabilized with hardware.
Sagittal split osteotomy is performed with prognathism, a condition in which the mandible is oversized, causing an underbite.
This procedure is performed by transecting the mandible bilaterally, repositioning it in a more posterior position, and stabilizing it with hardware.
Mandibular fractures are most commonly caused by trauma.
Mandibular fractures typically occur in two places: the parasymphysis due to the incisive fossa and mental foramen.
A direct blow to the mandible may cause a condylar neck fracture at the articular disk of the temporomandibular joint.
In patients with traumatic mandibular injuries, a standard four-view series of X-ray film may not provide sufficient detail to accurately diagnose condylar fractures.
A reversed Towne view is more sensitive than X-ray.
CT imaging is commonly employed.
Dislocation of the mandible is most frequently in the posterior direction, but anterior and inferior dislocations may be observed, with the inability to close his or her mouth or with an asymmetric jawline.
Manual reduction is often used to correct the injury.
The mandible is a vital bone in terms of forensic evidence: it is routinely used to determine the age of the deceased.
The mandible constantly changes throughout life.: At birth, the gonial angle is approximately 160 degrees.
By age four, teeth have formed, causing the jaw to elongate and widen; these changes in the mandible’s dimensions cause the gonial angle to decrease to approximately 140 degrees.
By adulthood, the gonial angle is decreased to approximately 120 degrees.
Mandibular fractures are most commonly caused by trauma.
Fractures typically occur in two places: parasymphysis is especially prone to fracture due to the incisive fossa and mental foramen: a direct blow to the mandible may cause a condylar neck fracture as the articular disk of the temporomandibular joint prevents it from moving posteriorly.
The mandible progressively changes over an individual’s life, it is routinely used to determine the age of the deceased.
Males generally have squarer, stronger, and larger mandibles than females.
The mental protuberance is more pronounced in males.
The mandible forms as a bone (ossifies) over time from a left and right piece of cartilage, called Meckel’s cartilage.
One fifth of facial injuries involve a mandibular fracture.
Mandibular fractures are often accompanied by a twin fracture on the opposite side.
A common treatment involves attachment of metal plates to the fracture to assist in healing.
The causes of mandibular fractures:
Motor vehicle accident 40%
Assault 10%
Fall 10%
Sport 5%
Other 5%
The mandible may be dislocated anteriorly, inferiorly but very rarely posteriorly.
The mandibular alveolar process can become resorbed when completely edentulous in the mandibular arch
When remains of humans are found, the mandible is one of the common findings, and experts can estimate the age of the human upon death because the mandible changes over a person’s life.