 Refers to an increase in the number or proportion of lymphocytes in the blood.
Refers to an increase in the number or proportion of lymphocytes in the blood.
It is usually detected when a complete blood count is obtained.
Lymphocytes normally represent 20 to 40% of circulating white blood cells.
The absolute lymphocyte count can be directly measured by flow cytometry, or calculated by multiplying the total white blood cell count by the percentage of lymphocytes found in the differential count.
In absolute lymphocytosis, the total lymphocyte count is elevated above the population reference range.
In adults, absolute lymphocytosis is present when the absolute lymphocyte count is greater than 4000 per microliter.
In older children greater than 7000 per microliter and in infants greater than 9000 per microliter is considered absolute lymphocytosis.
Relative lymphocytosis occurs when there is a higher proportion of lymphocytes among the white blood cells, however, absolute lymphocyte count is normal.
Relative lymphocytosis is normal in children under age 2.
Caused by a variety of infections and diseases.
Viral infections are the most common cause of lymphocytosis,
Infection mononucleosis generally affects adolescents and young adults and is spread through blood and saliva with common systems include sore throat, fever, and fatigue.
Bacterial infections such as tuberculosis can also cause lymphocytosis.
Blood diseases such as chronic lymphocytic leukemia and other forms of leukemia are also possible causes of lymphocytosis.
Lymphocytosis is defined in most laboratories as an absolute lymphocyte count greater than 4.0 × 109/L for adults.
Lymphocytosis is usually caused by infection, but it can have other causes, including malignancy.
Normally, T cells (CD3+) make up 60% to 80% of lymphocytes, B cells (CD20+) 10% to 20%, and natural killer (NK) cells (CD3–, CD56+) 5% to 10%.
A peripheral blood smear can be used to assess lymphocyte morphology, providing clues to the underlying etiology: atypical lymphocytes are often seen in infectious mononucleosis, while “smudge” lymphocytes are characteristic of chronic lymphocytic leukemia.
If a peripheral smear shows abnormal morphology, further workup should include establishing whether the lymphocytes are polyclonal or clonal.
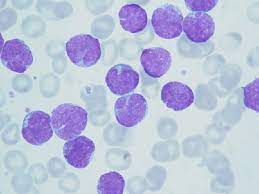
Case continued: Large granular lymphocytes
Large lymphocytes with moderate amounts of pale cytoplasm filled with azurophilic granules, consistent with large granular lymphocytes.
Flow cytometry analysis is the best first test to determine the cause of lymphocytosis after review of the peripheral smear.
For persistent lymphocytosis, flow cytometry should be done.
Most T cells possess receptors composed of alpha and beta chains, encoded by variable gene segments, which undergo rearrangement during T-cell development in the thymus based on antigen exposure, producing a diverse T-cell receptor population.
In a polyclonal population of lymphocytes, the T-cell receptors have a variety of gene segment arrangements, typicalmofna normal T-cell development.
In a clonal population of lymphocytes, the T-cell receptors have a single identical gene segment arrangement, indicating they all originated from a single clone.
Lymphocytosis in response to an infection is typically polyclonal, while malignant lymphocytosis is clonal.
Flow cytometry can establish clonality.
T-cell receptor gene rearrangement studies can also be performed using polymerase chain reaction and Southern blot techniques.