 Circulate in the blood and lymph but also accumulates in lymph nodes, thymus, spleen, tonsils, adenoids, and Peyer patches.
Circulate in the blood and lymph but also accumulates in lymph nodes, thymus, spleen, tonsils, adenoids, and Peyer patches.
Lymphocytes have long life spans, nearly 80 percent survive for four years and some last as much as 20 years or more.
Produced in the bone marrow and lymphoid tissues.
The absolute lymphocye count (ALC) <350 cells/mcgL during induction predicts for poor prognosis in ALL or AML in children or young adults.
Lymphocytosis is defined in most laboratories as an absolute lymphocyte count greater than 4.0 × 109/L for adults.
Lymphocytosis is usually caused by infection, but it can have other causes, including malignancy.
Normally, T cells (CD3+) make up 60% to 80% of lymphocytes, B cells (CD20+) 10% to 20%, and natural killer (NK) cells (CD3–, CD56+) 5% to 10%.
A peripheral blood smear can be used to assess lymphocyte morphology, providing clues to the underlying etiology: atypical lymphocytes are often seen in infectious mononucleosis, while “smudge” lymphocytes are characteristic of chronic lymphocytic leukemia.
If a peripheral smear shows abnormal morphology, further workup should include establishing whether the lymphocytes are polyclonal or clonal.
Decreased numbers or function of lymphocytes reduce ability of immune system to respond to cancer cells.
Autologous T and natural killer (NK) cells play a role in maintaining remission in AML.
Higher lymphocyte counts predict improved survival in patients that have undergone autologous or allogeneic transplantation for a number of malignancies.
Include natural killer cells (NK cells), which function in cell-mediated, cytotoxic innate immunity, T cells ,for cell-mediated, cytotoxic adaptive immunity, and B cells,for humoral, antibody-driven adaptive immunity.
They are the main type of cells found in lymph.
The three major types of lymphocyte are T cells, B cells and natural killer (NK) cells.
T cells (thymus cells) and B cells (bone marrow- or bursa-derived cells are the major cellular components of the adaptive immune response.
T cells are involved in cell-mediated immunity, whereas B cells are primarily responsible for humoral immunity.
The function of T cells and B cells is to recognize specific non-self antigens, during antigen presentation.
Lymphocyte development and priming is most active in fetal development but continues throughout life as immature lymphocytes are generated, slowing as the thymus degenerates and the bone marrow shrinks in adult life.
Once they have identified an invader, lymphocytic cells generate specific responses to eliminate specific pathogens or pathogen-infected cells.
B cells respond to pathogens by producing antibodies which then neutralize foreign objects like bacteria and viruses.
Some T cells, called T helper cells, produce cytokines that direct the immune response.
Other T cells, called cytotoxic T cells, produce toxic granules that contain enzymes which induce the death of pathogen-infected cells.
Following activation, B cells and T cells leave a lasting antigen memory.
Memory cells will remember each specific pathogen encountered, and are able to mount a strong and rapid response if the pathogen is detected again.
NK cells are a part of the innate immune system and play a major role in defending the host from both tumors and virally infected cells.
NK cells distinguish infected cells and tumors from normal and uninfected cells by recognizing changes of a surface molecule called MHC (major histocompatibility complex) class I.
NK cells are activated in response to a family of cytokine interferons.
Activated NK cells release cytotoxic granules which then destroy the altered cells.
Natural killer cells do not require prior activation in order to kill cells which are missing MHC class I.
All lymphocytes originate from a common lymphoid progenitor before differentiating into their distinct lymphocyte types.
The formation of lymphocytes is known as lymphopoiesis.
B cells mature into B lymphocytes in the bursa equivalent, which is thought to be located in the Peyer’s patches of the intestine, while T cells migrate to and mature in the thymus.
Following maturation, the lymphocytes enter the circulation and peripheral lymphoid organs where they survey for invading pathogens and/or tumor cells.
The lymphocytes involved in adaptive immunity such as B and T cells differentiate after exposure to an antigen, forming effector and memory lymphocytes.
Effector lymphocytes eliminate the antigen, either by releasing antibodies by B cells, cytotoxic granules by T cells or by signaling to other cells of the immune system known as helper T cells.
Memory T cells remain in the peripheral tissues and circulation for an extended time ready to respond to the same antigen upon future exposure.
Memory T cells live weeks to several years to a whole lifetime.
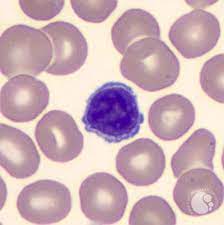
Lymphocytes have a coarse, dense nucleus.
The nucleus of a lymphocyte is approximately the size of a red blood cell, about seven micrometres in diameter.
Some lymphocytes show a halo around the nucleus or could exhibit a small clear zone to one side of the nucleus.
Polyribosomes are a prominent in the lymphocytes and can be viewed with an electron microscope.
Ribosomes are involved in protein synthesis of large quantities of cytokines and immunoglobulins by these cells.
It is not possible to distinguish between T cells and B cells on a peripheral blood smear.
Flow cytometry testing is used to determine the percentage of lymphocytes that contain a particular combination of specific cell surface proteins, such as immunoglobulins or cluster of differentiation (CD) markers or that produce particular proteins.
Natural killer cells can result in lysis of virally infected cells and tumor cells and comprise about 7% of lymphocytes.
T helper cells release cytokines and growth factors that regulate other immune cells and account for approximately 46% of lymphocytes.
Cytotoxic T cells lyse virally infected cells, tumor cells and allografts and make up approximately 19% of cells.
Gamma delta T cells provide immunoregulation and cytotoxicity and make up about 5% of lymphocytes.
B cells provide secretion of antibodies and make up 23%.
In the circulatory system, lymphocytes move from lymph node to lymph node.
Macrophages are rather stationary in the nodes.
A lymphocyte count is usually part of a peripheral complete blood cell count and is expressed as the percentage of lymphocytes to the total number of white blood cells counted.
A general increase in the number of lymphocytes is known as lymphocytosis, whereas a decrease is known as lymphocytopenia.
An increase in lymphocyte concentration is usually a sign of a viral infection.
A high lymphocyte count with a low neutrophil count might be caused by leukemia or lymphoma.
A low normal to low absolute lymphocyte concentration is associated with increased rates of infection following surgery or trauma.
Low T cell lymphocyte levels occur when the human immunodeficiency virus (HIV) infects and destroys T cells.
HIV specifically destroys the CD4+ subgroup of T lymphocytes making patients susceptible to opportunistic infections that otherwise would not affect healthy people.
The extent of HIV progression is typically determined by measuring the percentage of CD4+ T cells in the patient’s blood.
HIV ultimately progresses to Acquired Immune Deficiency Syndrome (AIDS).
Tumor-infiltrating lymphocytes in some cancers, e.g., melanoma and colorectal cancer, lymphocytes can inhibit tumor growth.
Circulating lymphocytes have anti-tumor activity by inducing cytotoxic cell death and inhibiting tumor proliferation with increased infiltration into tissue predicting better search survival outcomes.