 Refer to diets of less than 60 g of carbohydrates daily.
Refer to diets of less than 60 g of carbohydrates daily.
A low-carbohydrate diet restricts the amount of carbohydrate-rich foods, such as bread, in the diet.
Some define low-carbohydrate diets as diets that restrict carbohydrate intake to 20 to 60 grams per day, typically less than 20% of caloric intake.
A 2016 review of low-carbohydrate diets classified diets with 50g of carbohydrate per day, less than 10% of total calories, as “very low” and diets with 40% of calories from carbohydrates as “mild” low-carbohydrate diets.
Any diet, in which carbohydrates contribute less than 40 to 45% of total energy intake, a percentage that is assumed to represent the average carbohydrate consumption, can be classified as low in carbohydrates.
Diets that restrict carbohydrates can commonly induce metabolic changes similar to those seen during starvation and include changes in plasma levels of free fatty acids, insulin, glucose, and ketone bodies.
A decrease in one particular macronutrient is always accompanied by a parallel increase in another macronutrient-lipids,proteins.
20% of patients with diabetes can obtain drug free remission with a low carbohydrate diet.
Others propose that a very low carbohydrate diet had less that 10% caloric intake from carbohydrate, a low carbohydrate diet less than 26%, a medium carbohydrate diet less than 45%, and a high carbohydrate diet more than 45%.
Studies of long-term diets of very low or low in carbohydrates result in weight loss that is equivalent to, not better than, that achieve with other diets that have higher carbohydrate content.
Randomized control styles trials have shown that low carbohydrate ketogenic diets effectively reduce cardiovascular risk factors levels of blood glucose, glycated hemoglobin, and certain, but not all blood lipids, especially in patients with overweight or obesity and type two diabetes.
There is only poor-quality evidence of the effect of different diets on reducing or preventing high blood pressure, but it suggests the low-carbohydrate diet is among the better-performing ones, while the DASH diet performs best.
Both high- and low-carbohydrate diets are associated with increased mortality.
Two meta-analyses have shown that low carbohydrate diets are associated with higher mortality, especially for those whose diets favored animal derived proteins and fat.
Carbohydrate restricted dieting concerns are, particularly, for micronutrient sufficiency, bone health and cancer risk.
One meta-analysis reported that adverse effects could include “constipation, headache, halitosis, muscle cramp and general weakness.
High-quality research shows no long-term weight loss advantage to a ketogenic diet over a low fat diet.
There is a lack of data about long-term safety, and low-carbohydrate intake may be associated with increased mortality.
The optimal proportion of carbohydrate in a diet for health is thought to be 50-55%.
The National Academy of Medicine recommends a minimum intake of 130 g of carbohydrate per day.
The FAO and WHO similarly recommend that the majority of dietary energy come from carbohydrates.
Inadequate carbohydrate intake during athletic training causes metabolic acidosis, which may be responsible for the impaired performance which has been observed.
For people with metabolic conditions, in general a diet with approximately 40-50% high-quality carbohydrate is compatible with what is scientifically established to be a healthy diet.
Low-carbohydrate diet proponents emphasize low-carbohydrate diets can initially cause slightly greater weight loss than a balanced diet, but any such advantage does not persist.
There is no good evidence that low carbohydrate/high fat diets offer a superior diet choice to a more conventional healthy diet, as recommended by many health authorities, in which carbohydrate typically accounts for more than 40% of calories consumed.
Much of the research into low-carbohydrate dieting has been of poor quality.
A low-carbohydrate diet has been found to reduce endurance capacity for intense exercise efforts, and depleted muscle glycogen following such efforts is only slowly replenished if a low-carbohydrate diet is taken.
Higher quality studies tend to find no meaningful difference in outcome between low-fat and low-carbohydrate dieting.
An American Journal of Clinical Nutrition study did not provide convincing evidence of any advantage to a low-carbohydrate diet as compared to diets of other composition – ultimately a very low-calorie, ketogenic diet (of 5% carbohydrate) was not associated with significant loss of fat mass compared to a non-specialized diet with the same calories; there was no useful metabolic advantage.
In the long-term successful weight maintenance is determined by calorie intake, and not by macronutrient ratios.
Studies have shown that people losing weight with a low-carbohydrate diet, compared to a low-fat diet, have very slightly more weight loss initially, equivalent to approximately 100kcal/day, but that the advantage diminishes over time and is ultimately insignificant.
When calorie intake is held constant body-fat accumulation does not appear to be affected by even very pronounced changes in the amount of fat vs carbohydrate in the diet.
It is unclear whether low-carbohydrate dieting had any beneficial effect on cardiovascular health, though such diets can cause high LDL cholesterol levels, which carry a risk of atherosclerosis in the long term.
Potential favorable changes in triglyceride and HDL cholesterol values should be weighed against potential unfavorable changes in LDL and total cholesterol values.
Some fruits may contain relatively high concentrations of sugar, most are largely water and not particularly calorie-dense.
Even sweet fruits and berries do not represent a significant source of carbohydrates in their natural form, and also typically contain a good deal of which attenuates the absorption of sugar in the gut.
Significantly restricting the proportion of carbohydrate in diet risks causing malnutrition, and can make it difficult to get enough dietary fiber to stay healthy.
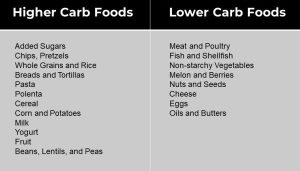
Foods high in carbohydrates- sugar, bread, pasta, are limited or replaced with foods containing a higher percentage of fats and moderate protein, such as meat, poultry, fish, shellfish, eggs, cheese, nuts, and seeds, and other foods low in carbohydrates, such as most salad vegetables such as spinach, kale, chard and collards.although other vegetables and fruits, especially berries, are often allowed.
Most vegetables are low- or moderate-carbohydrate foods.
In some low-carbohydrate diets, fiber is excluded because it is not a nutritive carbohydrate.
Some vegetables, such as potatoes, carrots, corn and rice are high in starch.
Most low-carbohydrate diet plans accommodate vegetables such as broccoli, spinach, kale, lettuce, cucumbers cauliflower, peppers and most green-leafy vegetables.
There is a lack of standardization of how much carbohydrate low-carbohydrate diets must have, and one definition, from the American Academy of Family Physicians, specifies low-carbohydrate diets as having less than 20% carbohydrate content.
The Atkins and South Beach diet start with less than 20 g of carbohydrates daily and increase with time.
Based on theory that a limited carbohydrate intake will force the body to use stored fat as fuel through ketosis, resulting in fat loss.
The state of ketosis induced by the diet can occasionally progress to ketoacidosis in healthy persons.
Ketoacidosis, which usually occurs only in diabetes, alcoholism or starvation, is a severe condition that requires immediate medical intervention.
Low-carb diets cause people to burn more calories
Most people regain their weight they lose from dieting within one or two years, in part, because of slowing metabolism and burning fewer calories.
Eating fewer carbohydrates increases the number of calories burned: Framingham State Food Study
Low-carb diets can help people maintain weight loss, making obesity treatment more effective.
Processed carbohydrates during the low-fat era have raised insulin levels, driving fat cells to store excessive calories.
There is evidence that the quality, rather than the quantity, of carbohydrate in a diet is important for health, and that choosing diet for health conditions should have their diet tailored to their individual requirements.
Most, but not all, trials indicate that in the first 6 months randomization between low carbohydrate and low fat diets, that the low carbohydrate diet yields significantly more weight loss in the first 6 months: at twelve months the differences were not significant.
It has been repeatedly found that in the long-term, all diets with the same calorific value perform the same for weight loss, except for the one factor of how well people can faithfully follow the dietary program.
A study comparing groups taking low-fat, low-carbohydrate and Mediterranean diets found at six months the low-carbohydrate diet still had most people adhering to it, but thereafter the situation reversed: at two years the low-carbohydrate group had the highest incidence of lapses and dropouts.
Compared to low fat diets result in lower fasting blood sugar levels in individuals with diabetes, lower plasma triglycerides and higher HDL levels with an increase in LDL cholesterol.
There is no good evidence that low-carbohydrate dieting is helpful in the management of type 1 diabetes, and weak evidence that carbohydrate reduction in an otherwise healthy diet is helpful in managing type 2 diabetes.
Low-carbohydrate dieting has no effect on the kidney function of people who have type 2 diabetes.
Generally this type of diet avoids breads, pasta, rice, and other carbohydrates, but complex carbohydrates may be permitted in limited amounts.
These diets are associated with the greatest weight change from baseline after two months and can induce a rapid weight-loss that levels off and even increases slightly by 12 months.
Approximately 25% of individuals can sustain clinically significant weight loss, defined as weight loss of 5% of baseline body weight, after one year.
Such diets significantly increase HDL cholesterol up to 12 months from baseline with associated significant reductions in triglycerides, while some studies also show a significant decrease in low-density lipoprotein cholesterol.
These diet may also significantly reduce blood pressure both diastolic and systolic.
Among persons on a low carbohydrate diet, those who consume most of their fat and protein from vegetable sources have lower cardiovascular and all cause mortality rates.
Such diets can reduce fasting plasma glucose levels in the short-term and can reduce plasma insulin levels.
Low-carb diets cause people to burn more calories.
Low-carbohydrate diets are associated with increased mortality, and they can miss out on the health benefits afforded by high-quality carbohydrate such as is found in fruit and vegetables.
Disadvantages of the diet might include halitosis, headache and constipation, and in general the potential adverse effects of the diet are under-researched, particularly for more serious possible risks such as for bone health and cancer incidence.
It is not clear how low-carbohydrate dieting affects cardiovascular health; any benefit from HDL cholesterol might be offset by raised LDL cholesterol, which risks causing clogged arteries in the long term.
Carbohydrate-restricted diets are no more effective than a conventional healthy diet in preventing the onset of type 2 diabetes, but for people with type 2 diabetes they are a viable option for losing weight or helping with glycemic control.
Carbohydrate-restricted dieting does not appear to be helpful in managing type 1 diabetes.
The American Diabetes Association recommends that people with diabetes should adopt a generally healthy diet, rather than a diet focused on carbohydrate or other macronutrients.
Most people regain the weight they lose from dieting within one or two years, in part because the body adapts by slowing metabolism and burning fewer calories.
Eating fewer carbohydrates increases the number of calories burned: Framingham State Food Study
Low-carb diets can help people maintain weight loss, making obesity treatment more effective.
Processed carbohydrates during the low-fat era have raised insulin levels, driving fat cells to store excessive calories.
With fewer calories available to the rest of the body, hunger increases and metabolism slows, causing weight gain.
Participants randomized to follow high-, moderate- or low-carbohydrate diets, with carbs comprising 60, 40 and 20 percent of total calories, respectively.
The goal in the above study was to compare energy expenditure―how the different groups burned calories at the same weight.
Over the 20 weeks, total energy expenditure was significantly greater on the low-carbohydrate diet versus the high-carbohydrate diet.
Participants who consumed the low-carb diet burned about 250 kilocalories a day more than those on the high-carb diet.
In people with the highest insulin secretion at baseline, the difference in calorie expenditure between the low- and high-carb diets was even greater, about 400 kilocalories per day.
Ghrelin, which reduces calorie burning, was significantly lower on the low- versus high-carb diet.
The study suggested low-carb diets also decrease hunger, which could help with weight loss in the long term.
Leafy vegetables are low in carbohydrates.
The ketogenic diet is an established as a medical diet for treating epilepsy.
The ketogenic diet is an extreme form of a low-carbohydrate diet.
It is a popular weight-loss fad diet, but there is no evidence of any distinctive benefit for this purpose, and it risks causing a number of side effects.