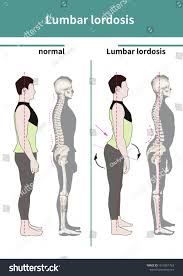
 Lordosis is defined as an abnormal inward curvature of the lumbar spine.
Lordosis is defined as an abnormal inward curvature of the lumbar spine.
Lordosis and lordotic are also used to refer to the normal inward curvature of the lumbar and cervical regions of the human spine.
Kyphosis historically refers to abnormal convex curvature of the spine.
The normal outward convex curvature in the thoracic and sacral regions is also termed kyphosis or kyphotic.
Lordosis makes it easier to bring the bulk of mass over the pelvis.
allowing for a much more efficient walking gait than that of other primates, whose inflexible spines cause them an inefficient forward leaning bent-knee, bent-waist gait.
Lordosis is one of the primary physiological adaptations of the human skeleton that allows for human gait to be as energetically efficient as it is.
Lumbar hyperlordosis is excessive extension of the lumbar region, and is commonly called hollow back, sway back, or saddle back.
Normal lordotic curvatures, result in a difference in the thickness between the front and back parts of the intervertebral disc.
Lordosis increase at puberty.
Lumbar hyperlordosis is a condition that occurs when the lumbar region experiences stress or extra weight and is arched to point of muscle pain or spasms.
Lumbar hyperlordosis occurs when the natural curve of the lumbar region of the back is slightly or dramatically accentuated.
Lumbar lordosis is known as swayback, and it is common in dancers.
Lumbar lordosis is a common pattern of posture dysfunction that differs from normal posture in the following ways:
The hips and pelvis are tilted forward in front of the head line.
The forward shift of the pelvis causes an exaggerated inward curve of the lower back or lumbar spine.
It also causes an exaggerated outward curve of the upper back, called kyphosis.
The misalignment of the spine and pelvis from swayback posture can increase risk of developing back and hip injuries.
Lordosis can contribute to musculoskeletal injuries in other parts of the body forced into a compromised position, such as the neck and shoulders.
Poor posture can also put pressure on your internal organs resulting in
constipation, heartburn and incontinence.
Imbalances in muscle strength and length are also a cause of lordosis, such as weak hamstrings, or tight hip flexors.
Lumbar hyperlordosis manifests as a forward pelvic tilt, resulting in the pelvis resting on top of the thighs.
Hyperlordosis can also be caused by:
Achondroplasia
Spondylolisthesis
Osteoporosis
Obesity,
Hyperkyphosis
Discititis
Benign juvenile lordosis.
Rare diseases, as is the case with Ehlers Danlos Syndrome (EDS), where hyper-extensive and usually unstable joints.
Excessive lordotic curvature (lumbar hyperlordosis) is also called hollow back and saddle back.
Common causes of lumbar hyperlordosis include tight low back muscles, excessive visceral fat, and pregnancy, and Rickets in children, can cause lumbar hyperlordosis.
Lumbar hypolordosis is less common than lumbar hyperlordosis.
Hypolordosis (flatback) occurs when there’s less of a curve in the lower back or a flattening of the lower back.
With hypolordosis the vertebrae are oriented toward the back of the spine, stretching the disc towards the back and compressing it in the front, causing a narrowing of the opening for the nerves, potentially pinching them.
Lumbar hyperlordosis, or anterior pelvic tilt, impacts height of individuals suffering from this medical issue, a height loss of 0.5–2.5 inches (1.27–6.35 centimeters) is common.
Transfeminine people have weaker muscles in the lower back due to increased estrogen intake and other such treatments, and associated with height loss.
Height loss can be due to a genetic condition, trauma to the spine, pregnancy in women, increased abdominal fat or a sedentary lifestyle.
Slouching does not cause height loss,
whereas lumbar hyperlordosis leads to actual and measured height loss.
Lumbar hyperlordosis can lead to moderate to severe lower back pain.
X-rays are used to measure the lumbar curvature.
On a lateral X-ray, a normal range of the lordotic curvature of between 20° and 60°, as measured from the inferior endplate of T12 to the inferior endplate of L5: a range of 40° and 60° as measured between the upper endplate of Th12 and the upper endplate of S1:
The lordotic curvature is generally more pronounced in females.
The lordotic curvature is relatively constant through adolescence and young adulthood, but decreases in the elderly.
TREATMENT:
Corrective exercises can be done to alleviate lordosis.
Since lumbar hyperlordosis is usually caused by habitual poor posture, rather than by an inherent physical defect like scoliosis or hyperkyphosis.
Lumbar lordosis can be reversed, by stretching the lower back, hip-flexors, quads and strengthening the abdominal muscles, hamstrings and glutes.
Strengthening the gluteal complex is a commonly accepted practice to reverse excessive lumbar lordosis, as an increase in gluteals muscle tone assist in the reduction excessive anterior pelvic tilt and lumbar hyperlordosis.
Intra-articular hip pain has been shown to inhibit gluteal contraction potential and could be a main contributing factor to gluteal inhibition.
Lumbar hyperlordosis may be treated by strengthening the hip extensors on the back of the thighs, and by stretching the hip flexors on the front of the thighs.
The muscles on the front and on the back of the thighs can rotate the pelvis forward or backward while in a standing position: discharging the force on the ground through the legs and feet.
Back hyper-extensions can strengthen all the posterior chain and will treat hyperlordosis, as will stiff legged deadlifts and supine hip lifts and any other similar movement strengthening the posterior chain without involving the hip flexors in the front of the thighs.