 Invasive, lobular, carcinoma accounts, for 10% of all breast cancers.
Invasive, lobular, carcinoma accounts, for 10% of all breast cancers.
Second most common histologic breast cancer.
It is increasing faster than other types of breast cancers among US women.
New cases are climbing at a rate of nearly 3% per year, compared with less than one percent for all of the breast cancers.
In 2021 14 cases per hundred thousand women with invasive lobular carcinoma were reported accounting for 10% of breast cancer cases.
Rising incidence may be due to increase alcohol consumption, excessive body, weight, and later ages of first birth or menopause.
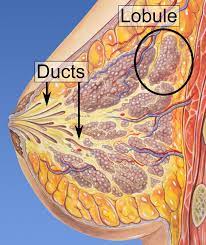
More difficult to palpate and more likely to be missed on mammograms than ductal carcinoma of the breast.
Classic lobular BC is hormone receptor positive and HER2 negative BC.
Mostly represented by luminal A, or low proliferative tumors, followed by luminal B, or high proliferative tumors.
The majority (93%) of metastatic lobular carcinomas are hormone receptor positive and HER2 negative.
Tends to be larger than infiltrating ductal cancer at diagnosis with an average size of 29 mm.
Associated with older age compared to invasive ductal cancer.
Its biological hallmark is the loss of cell adhesion molecule E-cadherin, which explains elevated instance of metastasis to unusual sites, such as the G.I. tract, pelvic organs, and retroperitoneum.
There is loss of the cell adhesion proteins E-cadherin in approximately 90% of cases because of the loss of function via genomic most commonly of 16q or mutation.
Inherited mutations in the CDH1 gene increase a woman’s risk of developing a lobular breast cancer.
Typically has a low-intermediate histologic grade and is often estrogen receptor positive, progesterone receptor positive, and HER2 negative.
Infiltrating LC generally has features associated with a good prognosis: low grade, low, proliferation index, and strong ER positivity.
LC tends to higher risk of distant recurrence after 10 years, and exhibits unusual metastatic patterns, compared to infiltrating ductal carcinoma.
It is more difficult to perform successful breast conserving surgery in such patients as the lesions are often associated with vague densities on clinical exam as well as on imaging, making margin control more difficult.
If negative margins can be controlled the local control of invasive lobular cancers is comparable to that of ductal cancers.
The presence of lobular carcinoma in situ coexisting with invasive cancer does not affect rates of local recurrence.
Can be diagnosed from stages 1 through 4.
More likely than Infiltrating ducal cancer to occur in both breasts.
About 20% of patients diagnosed with ILC will have bilateral breast cancer.
Calcifications are uncommon on mammography.
Local recurrence rate 3-5% at 5 years and 7% at 10 years when treated with conservative surgery and radiation therapy, rates comparable with infiltrating ductal carcinoma.
Extent of disease is often grossly underestimated.
Greater rate of contralateral breast cancer compared to infiltrating ductal carcinoma.
The risk of contralateral disease does not warrant mirror image contralateral biopsies.
More prone to develop leptomeningeal metastases than other types of breast cancer.
Lobular carcinoma tumors do not respond well to neoadjuvant therapy, as response rates are low and chance for large lesion to undergo conservative surgery is low.
As long as metastatic infiltrating, lobular carcinoma is hormone sensitive, they are treated with sequential lines of endocrine therapy and combination with targeted therapies such as cyclin dependent kinase is 4/6 inhibitors, m-TOR inhibitors everolimus, and the phoshpinositide 3-kinase inhibitors apelisib.
BIG 1-98 trial comparing the effectiveness of adjuvant letrozole to tamoxifen given for 5 years to post menopausal hormone receptor positive BC letrozole had a significant greater disease free survival.
Data suggest that Exemestane is less effective in lobular breast cancer than the two nonsteroidal AI’s anastrozole or letrozole.
Once refractory to hormonal therapy, most chemotherapy agents, including taxanes and capecitabine are used.