 Conduction of wave of depolarization in left ventricle is altered proceeding from the anterior septum through left myocardium to the inferior and lateral left ventricular walls.
Conduction of wave of depolarization in left ventricle is altered proceeding from the anterior septum through left myocardium to the inferior and lateral left ventricular walls.
The left bundle branch (LBB) is a vital part of the heart’s electrical conduction system that carries signals to the left ventricle, the heart’s main pumping chamber.
Results in left ventricular contracture dyssynchrony with the interventricular septum contracting before the left ventricular free wall.
When this pathway is damaged or blocked, it results in left bundle branch block (LBBB), which causes the left ventricle to contract slightly after the right ventricle.
LBBB is an electrical abnormality where the impulse to the left ventricle is delayed or blocked.
Left bundle branch block: LBBB affects about 0.06% to 0.1% of the U.S. population.
Left ventricular dyssynchrony results in mechanical inefficiency and decreased the left ventricular ejection fraction and cardiac output.
Because the LBB is blocked, the signal must travel through the heart muscle from the right side, which is much slower than the specialized conduction system.
One quarter to one third of patients with congestive heart failure have left bundle branch block.
The left bundle primarily receives blood from the left anterior descending and posterior descending arteries.
LBBB is rarely found in young, healthy individuals and is usually a marker of underlying heart disease.
Common causes:
Coronary Artery Disease: Including history of heart attack. Hypertension: Long-term high blood pressure that thickens the heart muscle. Cardiomyopathy: Weakening or enlargement of the heart muscle. Valvular Disease: Specifically aortic stenosis. Degenerative Aging: Fibrosis of the conduction system (Lev’s or Lenègre’s disease).
Approximately 6.7% of patients with an acute MI present with LBBB, which could interfere with EKG interpretation and diagnosis when the age of the LBBB is unknown.
Chest pain may not be present in up to half of patients with LBBB and acute MI (Shipak MG).
Left bundle branch area pacing improves patients with nonischemic cardiomyopathy, decreasing left ventricular and systolic volume and improving NYHA class function, narrowing of the QRS complex and clinical improvements in 72% of patients.
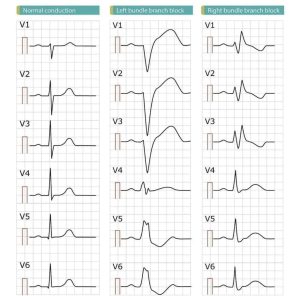
Diagnosis: It is primarily diagnosed via a 12-lead Electrocardiogram (ECG/EKG). Key criteria include a QRS duration ≥ 120 ms and specific wave patterns (notched R waves) in lateral leads (V5, V6, I, aVL).
Symptoms: Often asymptomatic, but can cause dizziness, fainting, or shortness of breath if it significantly impairs heart function.
Treatment:
Asymptomatic: If no other heart disease is present, treatment may not be required.
Heart Failure: For patients with heart failure and LBBB, Cardiac Resynchronization Therapy (CRT)—a specialized pacemaker—is often used to restore synchronized beating.
The natural history in humans progresses from isolated Left bundle branch block → HFpEF (heart failure with preserved ejection faction)→ HFmrEF (heart failure with moderate ejection fraction)→ HFrEF (heart failure with reduced ejection fraction) over 5–21 years. Left bundle branch block
Regular follow-ups with a cardiologist are recommended to monitor for progression or underlying issues.