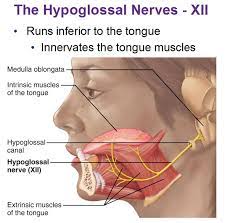
The hypoglossal nerve, also known as the twelfth cranial nerve, cranial nerve XII, or simply CN XII.
It is a cranial nerve that innervates all the extrinsic and intrinsic muscles of the tongue except for the palatoglossus.
The palatoglossus muscle is innervated by the vagus nerve.
CN XII nerve has a solely motor function.
The nerve arises from the hypoglossal nucleus in the medulla as a number of small rootlets.
The hypoglossal nucleus receives input from both the motor cortices but the contralateral input is dominant; innervation of the tongue is therefore essentially lateralized.
The nerve passes through the hypoglossal canal and down through the neck, and eventually passes up again over the tongue muscles it supplies into the tongue.
It innervates: genioglossus, hyoglossus, styloglossus, geniohyoid, thyrohyoid, intrinsic muscles of the tongue.
These represent all muscles of the tongue except the palatoglossus muscle.
The nerve controls the tongue movements required for speech and swallowing, including sticking out the tongue and moving it from side to side.
Damage to the nerve or the neural pathways affect the ability of the tongue to move and its appearance.
The most common types of damage are injury from trauma or surgery, and motor neuron disease.
The twelfth cranial arises as a number of small rootlets from the front of the medulla, the bottom part of the brainstem.
The rootlets of the hypoglossal nerve arise from the hypoglossal nucleus near the bottom of the brain stem.
It arises in the anterolateral sulcus which separates the olive and the pyramid.
The hypoglossal nerve passes through the subarachnoid space and pierces the dura mater near the hypoglossal canal, an opening in the occipital bone of the skull.
The hypoglossal nerve gives off a meningeal branch and picks up a branch from the anterior ramus of C1.
It travels close to the vagus nerve and spinal division of the accessory nerve.
It spirals downwards behind the vagus nerve and passes between the internal carotid artery and internal jugular vein lying on the carotid sheath.
At the angle of the mandible, the hypoglossal nerve emerges from behind the posterior belly of the digastric muscle, loops around a branch of the occipital artery and travels forward into the region beneath the mandible.
It moves forward lateral to the hyoglossus and medial to the stylohyoid muscles and lingual nerve, deep to the genioglossus muscle and continues forward to the tip of the tongue.
It distributes branches to the intrinsic and extrinsic muscle of the tongue:innervates hyoglossus, genioglossus and styloglossus as it passes.
Muscle spindles present on the tongue travel through the hypoglossal nerve, lingual nerve which synapse on the trigeminal mesencephalic nucleus.
Neurons of the hypoglossal nucleus are derived from the basal plate of the embryonic medulla oblongata.
The hypoglossal nerve provides motor control of the extrinsic muscles of the tongue: genioglossus, hyoglossus, styloglossus, and the intrinsic muscles of the tongue.
These muscles are involved in moving and manipulating the tongue.
The left and right genioglossus muscles are responsible for protruding the tongue.
The muscles, attached to the underside of the top and back parts of the tongue, cause the tongue to protrude and deviate towards the opposite side.
The hypoglossal nerve is of a general somatic efferent (GSE) type.
It supplies movements for clearing the mouth of saliva and other involuntary activities.
The hypoglossal nucleus interacts with the reticular formation, controlling reflex or automatic motions, and several corticonuclear originating fibers supply innervation aiding in unconscious movements related to speech/articulation.
Damage to the hypoglossal nerve is rare:compression by tumors and gunshot wounds, are the most common reasons.
Other causes: surgical damage, medullary stroke, multiple sclerosis, Guillain-Barre syndrome, infection, sarcoidosis, and presence of an ectatic vessel in the hypoglossal canal.
Damage can be on one or both sides.
It has close proximity to other structures including nerves, arteries, and veins, and it is rare for the nerve to be damaged in isolation.
Damage to the left and right hypoglossal nerves may occur with damage to the facial and trigeminal nerves as a result of a clot following arteriosclerosis of the vertebrobasilar artery.
Such a stroke may result in speaking, eating and chewing difficulties.
The motor neuron disease progressive bulbar palsy, is associated with combined lesions of the hypoglossal nucleus and nucleus ambiguus with atrophy of the motor nerves of the pons and medulla.
Motor neuron disease is the most common disease affecting the hypoglossal nerve, and causes difficulty with tongue movements, speech, chewing and swallowing caused by dysfunction of several cranial nerve nuclei.
An injured hypoglossal nerve will cause the tongue to atrophy and the tongue will not be able to stick out straight.
The hypoglossal nerve is tested by examining the tongue and its movements.
If the XII cranial nerve is injured a tongue may appear to have the appearance fasciculations or wasting.
Damage to the nerve or its pathways, will manifest as: tongue deviation to one side; make the the tongue feel thick, heavy,or clumsy; result in slurred speech, and affecting sounds.
Tongue strength may be tested by poking the tongue against the inside of their cheek, while an examiner feels or presses from the cheek.
The hypoglossal nerve carries lower motor neurons that synapse with upper motor neurons at the hypoglossal nucleus.
Damage is to the nerve itself is a lower motor neuron lesion, causing the tongue to curve toward the damaged side: weakness of the genioglossus muscle of affected side which action is to deviate the tongue in the contralateral side .
Damage is to the nerve pathway as an upper motor neuron lesion, the tongue will curve away from the side of damage, due to action of the affected genioglossus muscle, and with speech difficulties.
Damage to the hypoglossal nucleus leads to wasting of muscles of the tongue and deviation towards the affected side when it is stuck out.
The hypoglossal nerve may be anastomosed to the facial nerve to attempt to restore function when the facial nerve is damaged.