 Hyperammonemia is a life-threatening metabolic condition characterized by elevated levels of ammonia in the blood.
Hyperammonemia is a life-threatening metabolic condition characterized by elevated levels of ammonia in the blood.
Ammonia is a toxic byproduct of protein digestion that is normally converted into urea by the liver and excreted through urine; when this process fails, ammonia can build up and cross the blood-brain barrier, causing severe neurological damage.
Hyperammonemia is generally classified into two categories:
Acquired (Most Common in Adults): Approximately 90% of adult cases are caused by liver disease (such as cirrhosis or hepatitis), where the liver is too damaged to process ammonia.
Other causes include kidney failure, certain medications (like valproic acid, and infections with urease-producing bacteria.
Congenital (Most Common in Newborns): These are [inborn errors of metabolism, specifically urea cycle disorders (UCDs), where a child is born lacking one of the enzymes needed to convert ammonia to urea.
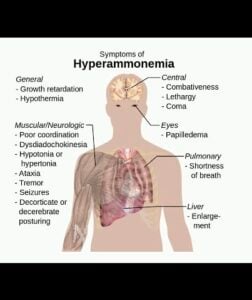
Symptoms are primarily neurological and can escalate rapidly into a medical emergency.
Newborns -Irritability, poor feeding, vomiting, seizures, grunting breath, coma.
Children/Adults | Nausea, headache, behavior changes, Confusion, asterixi, seizures, coma.
Diagnosis and Treatment: Ammonia-levels diagnose the condition.
Normal levels are typically below 35–50 µmol/L, while levels above 100–200 µmol/L are associated with severe symptoms.
Management:
Immediate treatment often involves stopping protein intake and providing high-calorie glucose solutions to prevent further ammonia production.
Ammonia Removal: For extremely high levels, hemodialysis is used to physically clean the blood.
Medications: Lactulose: A sugar that traps ammonia in the gut to be expelled through bowel movements.
Nitrogen Scavengers: Medications like sodium benzoate or phenylbutyrate help the body bypass the urea cycle to excrete nitrogen.
Antibiotics: Drugs like rifaximin may be used to reduce ammonia-producing bacteria in the intestines.