 The great saphenous vein is a large, subcutaneous, superficial vein of the leg.
The great saphenous vein is a large, subcutaneous, superficial vein of the leg.
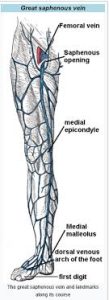
It is the longest vein in the body, running along the length of the lower limb, returning blood from the foot, leg and thigh to the deep femoral vein at the femoral triangle.
The great saphenous vein originates from where the dorsal vein of the big toe merges with the dorsal venous arch of the foot.
The saphenous vein passes in front of the medial malleolus, where it often can be visualized and palpated, it runs up the medial side of the leg.
At the knee, it runs over the posterior border of the medial epicondyle of the femur bone.
In the proximal anterior thigh 3–4 centimetres inferolateral to the pubic tubercle, the great saphenous vein dives down deep through the cribriform fascia of the saphenous opening to join the femoral vein.
It forms an arch, the saphenous arch, to join the common femoral vein in the region of the femoral triangle at the sapheno-femoral junction.
Superficial veins drain into the great saphenous and femoral vein.
Several veins join the great saphenous vein.
At the ankle, the great saphenous vein receives branches from the sole of the foot through the medial marginal vein.
In the lower leg it anastomoses freely with the small saphenous vein, communicates by perforator veins with the anterior and posterior tibial veins and receives many cutaneous veins.
Near the knee it communicates with the popliteal vein, in the thigh it communicates with the femoral vein by perforator veins and receives numerous tributaries; those from the medial and posterior parts of the thigh frequently unite to form a large accessory saphenous vein which joins the main vein near the sapheno-femoral junction.
Near the fossa ovalis it is joined by the superficial epigastric, superficial circumflex iliac vein, and superficial external pudendal veins.
There is an important communication between the femoral vein and the axillary vein.
Pathology of the great saphenous vein is relatively common, but is typically not life-threatening.
The great saphenous vein, like other superficial veins, can become varicose; swollen, twisted and lengthened, and unsightly.
Chronic venous insufficiency, can result in skin color changes in the calf and ulcers that may persist for years if the vein is not ablated.
The GSV can thrombosis and is usually not life-threatening in isolation; it can migrate to the deep venous system and to the pulmonary circulation.
GSV can be associated with, or progress to a deep vein thrombosis.
The vein is often removed by cardiac surgeons and used for autotransplantation in coronary artery bypass operations, when arterial grafts are not available or many grafts are required, such as in a triple bypass or quadruple bypass.
It is the conduit of choice for vascular, when available, for performing peripheral arterial bypass operations.
The saphenous vein graft failure after engraftment, has superior long-term patency compared to synthetic grafts, human umbilical vein grafts or biosynthetic grafts.
When emergency resuscitation with fluids is necessary, and standard intravenous access cannot be achieved due to venous collapse, saphenous vein cutdown may be a consideration.