 Genicular artery embolization (GAE) is a minimally invasive, outpatient procedure designed to relieve chronic knee pain from osteoarthritis by reducing blood flow to inflamed synovial tissue.
Genicular artery embolization (GAE) is a minimally invasive, outpatient procedure designed to relieve chronic knee pain from osteoarthritis by reducing blood flow to inflamed synovial tissue.
Genicular artery embolization (GAE) selectively embolizes hyperemic genicular artery branches to treat knee osteoarthritis (OA) pain refractory to conservative therapy and recurrent hemarthrosis after knee arthroplasty.
Performed by interventional radiologists under conscious sedation, GAE uses tiny particles to block abnormal vessels, offering significant pain reduction, improved mobility, and minimal downtime without surgery.
The procedure targets the pathologic neoangiogenesis and neoinnervation that drive synovial inflammation and pain in OA.
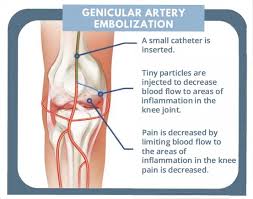
A small catheter is inserted, typically through the groin or wrist, and guided by X-ray to the knee’s genicular arteries.
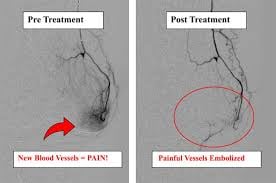
Selective catheterization of genicular artery branches is performed, and hyperemic target vessels are identified on digital subtraction angiography.
Microscopic particles are injected to block the vessels responsible for inflammation and pain signals.
Duration: The procedure typically takes about 90 minutes.
Candidates: Patients with chronic knee pain (osteoarthritis) who have not found relief through conservative treatments (e.g., physical therapy, medication) and wish to delay or avoid knee replacement.
Recovery: Most patients go home the same day and can resume light activities within 24 hours.
Results: significant pain reduction (50% or more) and improved functionality, with effects lasting over a year.
It is minimally Invasive: No general anesthesia is required.
Rapid Relief: Patients often experience decreased pain and swelling quickly.
No Damage to Joint: The procedure does not affect the main blood supply to the leg.
Risks and Side Effects
It is generally low-risk.
Possible, though uncommon, side effects include temporary skin changes (skin rash or discoloration) or, rarely, a small skin ulcer that can develop weeks after the procedure.
GAE has a favorable safety profile with no major adverse events reported in most prospective trials.
Minor adverse events include:
– Transient skin color changes (up to 50% of cases, associated with embolic volumes >3 mL)[9][8]
– Puncture-site hematoma (~10%)
– Mild postprocedural pain, typically resolving within 24 hours
Rare serious complications in the hemarthrosis population have included septic arthritis and aseptic necrosis of the femoral condyles.
GAE has a favorable safety profile with no major adverse events reported in most prospective trials.
Minor adverse events include:
– Transient skin color changes (up to 50% of cases, associated with embolic volumes >3 mL)[9][8]
– Puncture-site hematoma (~10%)
– Mild postprocedural pain, typically resolving within 24 hours
Rare serious complications in the hemarthrosis population have included septic arthritis and aseptic necrosis of the femoral condyles.
GAE works by arresting intra-articular neoangiogenesis, the abnormal new blood vessel formation that fuels the inflammatory cascade in OA.
By selectively embolizing hyperemic genicular branches corresponding to the site of knee pain, the procedure reduces blood flow to inflamed synovium and subchondral bone, thereby decreasing pathologic neoinnervation and pain signaling.
Biomarker studies have demonstrated reductions in serum VEGF, IL-1Ra, and nerve growth factor (NGF) following GAE, which may contribute to both pain relief and slowing of cartilage degeneration.
GAE is typically performed for patients with:
Knee OA pain refractory to conservative therapies of weight loss, physical therapy, NSAIDs, intra-articular glucocorticoid or gel injections, acetaminophen, tramadol, and/or radiofrequency nerve ablation for at least 6 months
Patients ineligible for or unwilling to undergo total knee arthroplasty
Recurrent hemarthrosis after knee arthroplasty
Current evidence most strongly supports benefit in mild-to-moderate OA though some data suggest efficacy in severe OA as well.
Prospective trials have reported clinical success rates of 62-83% (achieving minimal clinically important difference) at 12 months.
One study using gelatin sponge particles reported a 72% clinical success rate at 6 months.
Long-term durability beyond 12 months is not well characterized.
Outcomes are primarily based on subjective patient-reported measures
The embolization endpoint is described as the “pruning” technique with reduction of hypervascularity in target vessels while maintaining flow in parent vessels.
Embolic agents used include:
– Microspheres
– Polyvinyl alcohol (PVA) particles
Quick-soluble gelatin sponge particles