 Enteral nutrition is the following is providing essential entrance through an enteral tube to prevent or treat disease related malnutrition in patients who are unable to continue adequate nutrients by mouth.
Enteral nutrition is the following is providing essential entrance through an enteral tube to prevent or treat disease related malnutrition in patients who are unable to continue adequate nutrients by mouth.
Provides no advantage in preservation of gut barrier function, development of infectious complications, morbidity or mortality when energy and nitrogen intakes are similar.
Associated with fewer complications than parenteral nutrition and is less expensive to use.
Its use often, however, does not achieve caloric targets.
The main reason of non-use of EN is gastrointestinal intolerance ascribed to gastroparesis, with increased gastric volume, gastroesophageal reflux, regurgitation, vomiting, and risk of aspiration and ventilator associated pneumonoa.
Underfeeding critically ill patients is associated with weakness, infection, increased duration of mechanical ventilation and death.
Because patients cannot eat normally, artificial nutrition is often provided in patients with acute lung injury and with long duration of mechanical ventilation.
Enteral nutrition targeting full caloric needs is advocated over parenteral nutrition during mechanical ventilation.
Enteral nutrition is used in about 5% of malnourished hospitalized patients in the US.
Enteral nutrition is considered in patients with critical illness, dysphasia, neurologic, disease, gastrointestinal, or liver disease, cancer, cystic fibrosis, COPD and kidney disease.
Enteral nutrition is associated with improved clinical outcomes, fewer infections, shorter duration of mechanical ventilation, and lower mortality rates for patients receiving a higher percentage of calculated caloric needs.
Underfeeding with nutritional delivery of less than 70% of the calculated or measured energy requirements is hypothesized to support an adaptive metabolic response by allowing for ketogenesis, avoiding hyperglycemia, and promoting autophagic clearance of cellular damage.
The concept of improving recovery in critical illness is suggested by early energy and protein restriction.
Enteral nutrition and parenteral nutrition involving higher caloric intake are associated with harm, especially in patients with organ failure.
There is an association between a cumulative protein and energy deficit and worse outcomes in critical illness.
Intermittent or continuous feedings have similar outcomes in the number of stools per day and the likelihood of diarrhea or vomiting in critically ill children in pediatric intensive care units.
Vomiting occurs in approximately 6-12% of adult patients treated with continuous infusion nutrition.
The results of intermittent or continuous infusion feedings on the incidence of diarrhea have resulted in inconsistent results.
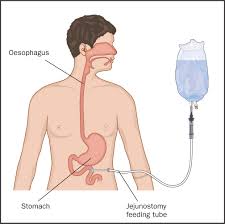
Early feeding with intraoperative jejunostomy is the preferred method for nutritional support of severely injured patients having surgery for multiple trauma.
Compared to parenteral nutrition results in a statistically reduced risk for infectious complications, pancreatic infections and mortality (Petrov).
Enteral nutrition use, as compared to parenteral nutrition in ICU patients is preferred when patients are able to do so.
Enteral nutrition contraindicated with diffuse peritonitis, intestinal obstruction, early stages of short bowel syndrome, paralytic ileus, intractable vomiting, severe gastrointestinal bleeding, severe diarrhea, high output fistulae, severe intestinal hemorrhages, intestinal ischemia, shock, and malabsorption syndromes.
Relative contraindications to use include pancreatitis and enterocutaneous fistulae.
A meta-analysis of intention-to-treat trials comparing enteral with parenteral nutrition in critically ill patients, revealed a reduction in mortality among patients receiving parenteral nutrition (Simpson F).
Randomized control trials of enteral nutrition in non-critically ill medical and surgical patient suggests the potential harm of under feeding: there was a significantly higher mortality at 90 days in the group receiving hypocaloric and nutrition then in a group receiving modified full nutrition.
In the above studies, if enteral nutrition was started within 24 hours of ICU admission no significant benefit was apparent for parenteral nutrition, and significant increases of infection occured in the parenteral nutrition group.(Simpson F).
13 randomized trials revealed that enteral nutrition in critically ill adult patients was associated with significant reductions in infectious complications compared to parenteral nutrition without a difference in mortality (Gramlich L).
Enteral nutrition in patients with mechanical ventilation indicate improved clinical outcomes, fewer infections, shorter duration of mechanical ventilation and lower mortality.
Hypocaloric feeding, or permissive underfeeding may result in shorter ventilation and improve mortality.
Trophic feedings, minimal amounts of enteral feedings, have beneficial effects in preserving intestinal epithelium, stimulating secretion of brush border enzymes, enhancing immune functions, preserving epithelial cellular junctions, and preventing bacterial translocation, despite not meeting daily calorie requirements.
In a randomized study with acute lung injury patients on mechanical ventilation receiving trophic versus full enteral nutrition: there was no difference in ventilator free days, 60 day mortality, or infectious complications but was associated with less gastrointestinal intolerance (EDEN randomized trial.
Augmenting enteral protein is proposed as it intervention to attenuate muscle atrophy and weakness and improve outcomes from critical illness: augmenting enteral protein for patients in the ICU does not improve outcomes.
Enteral studies in nutrition in surgical patients found that the amount of energy provided in the postoperative period affects outcomes.
The advantages of early as compared with late commencement of entering nutrition in surgical patient has been demonstrated: early supplemental paren nutrition started on postoperative day three versus late supplemental parenteral nutrition, started on postoperative day eight was associated with greater energy delivery and significantly fewer nosocomial infections.
Short term enteral access for duration of up to six weeks is typically through the nostrils, with the tip of the tube terminating in the stomach or beyond the pylorus in the duodenum or jejunum.
Postpyloric feeding may benefit patients who cannot receive feedings by the gastric route.
Postpyloric feedings are associated with a lower incidence of pulmonary aspiration, gastric, reflux, and pneumonia and a shorter time to reach nutritional targets.
Percutaneous gastric, percutaneous gastric, jejunal tubes can be placed in endoscopically, surgically or radiologically.
Small bore tubes made of silicone with polyurethane are softer and more comfortable than large-bore tubes but may be prone to clogging.
Large-bore (14 French) facilitate aspiration of gastric contents.
If enteral nutrition is needed for more than 4 to 6 weeks, placement of a long-term feeding tube is considered.
Enteral feeding formulas generally should provide macronutrient delivery of at least 1500 kcal per day.
Pump assisted continuous feeding is the most common method of delivering enteral nutrition.
Enteral nutrition is usually infused at a constant rate, but volume based feeling method may be efficacious.