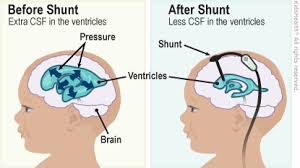
 CSF (cerebrospinal fluid) shunts are medical devices surgically implanted to treat hydrocephalus – a condition where excess cerebrospinal fluid accumulates in the brain’s ventricles.
CSF (cerebrospinal fluid) shunts are medical devices surgically implanted to treat hydrocephalus – a condition where excess cerebrospinal fluid accumulates in the brain’s ventricles.
The shunt redirects this fluid from the brain to another part of the body where it can be absorbed.
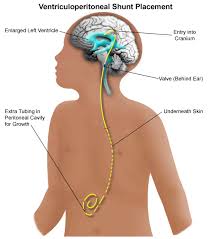
A typical shunt system consists of three parts: Proximal catheter that is inserted into the brain ventricle to drain CSF
Valve that regulates the flow rate and pressure of CSF drainage
Distal catheter that carries fluid to the drainage site-usually the abdominal cavity)
Common Types:
Ventriculoperitoneal (VP) shunt is the most common type, drains CSF from brain ventricles to the peritoneal cavity in the abdomen
Ventriculoatrial (VA) shunt-drains CSF to the right atrium of the heart; used when VP shunt isn’t feasible
Ventriculopleural shunt drains to the pleural space around the lungs; less common
Lumboperitoneal (LP) shunt drains from the lumbar spine to the abdomen; used for specific conditions like idiopathic intracranial hypertension
Shunts can have different valve mechanisms:
Fixed-pressure valves- drain at a preset pressure level
Adjustable valves-can be reprogrammed non-invasively using magnets
Flow-regulated valves- control the rate of CSF drainage
Anti-siphon devices-prevent over-drainage when standing
Indications: CSF shunts are used to treat:
Congenital hydrocephalus Acquired hydrocephalus from brain injury, infection, tumors, or hemorrhage Normal pressure hydrocephalus (NPH) in elderly patients Idiopathic intracranial hypertension (pseudotumor cerebri) Post-surgical or post-infectious hydrocephalus
The shunt creates an alternative pathway for CSF to drain when the body’s natural absorption is impaired.
As CSF accumulates and pressure builds in the ventricles, the valve opens to allow fluid to flow through the catheter to the drainage site, where it’s reabsorbed into the bloodstream.
Shunt malfunction can occur due to blockage, disconnection, or mechanical failure; most common reason for revision surgery
Infection occurs in 5-15% of cases, typically within the first few months after surgery; may require shunt removal and antibiotics
Over-drainage can cause low-pressure headaches, subdural hematomas, or slit ventricle syndrome
Under-drainage can result in persistent hydrocephalus symptoms.
Mechanical problems include catheter migration, breakage, or disconnection
VP shunts, can include CSF pseudocyst, bowel perforation, or peritonitis.
Malfunction symptoms may include:
Headaches Nausea and vomiting Vision changes Lethargy or changes in consciousness Cognitive changes Seizures Return of original hydrocephalus symptoms
Patients with shunts require lifelong monitoring because:
Shunts can malfunction at any time
Many patients need multiple revisions over their lifetime
Children may outgrow catheters as they grow
Regular imaging (CT or MRI) may be needed to assess ventricle size
With proper shunt function and management, most patients with hydrocephalus can lead relatively normal lives.
The average shunt survival is about 8-10 years, though some last much longer and others require earlier revision.
Endoscopic third ventriculostomy (ETV) is a surgical alternative where a hole is created in the floor of the third ventricle to allow CSF to bypass the obstruction; not suitable for all types of hydrocephalus but avoids the need for a permanent shunt in successful cases.