““ 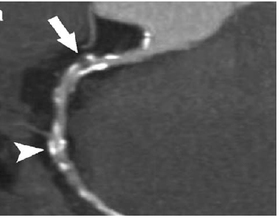
Coronary CT angiography is the use of computed tomography (CT) angiography to assess the coronary arteries of the heart.
The patient receives an intravenous injection of radiocontrast and then the heart is scanned using a high speed CT scanner, allowing assessment of the extent of occlusion in the coronary arteries, usually in order to diagnose coronary artery disease.
CTA is superior to coronary CT calcium scan in determining the risk of Major Adverse Cardiac Events (MACE).
It may be useful in the diagnosis of suspected coronary heart disease, for follow-up of a coronary artery bypass, for the evaluation of valvular heart disease and for the evaluation of cardiac masses.
Its greatest utility of cardiac CT lies in ruling out coronary artery disease rather than ruling it in. The use of coronary CT angiography unstable chest pain reduces costs and downstream interventions without compromising patient satisfaction, morbidity, or mortality.
It is highly sensitive for coronary artery disease,over 90% detection, so a negative test result largely rules out coronary artery disease.
CT coronary angiography is an accurate, noninvasive alternative to invasive coronary angiography in patients with stable chest pain and intermediate pretest probability for obstructive coronary artery disease.
CT coronary angiography used in patients with stable chest pain has improved prognostic value compared to exercise stress testing, resulting improved medical management.
Its greatest utility of cardiac CT lies in ruling out coronary artery disease rather than ruling it in.
Screening patients with stable chest pain with coronary CT angiography results in more appropriate percutaneous coronary interventions, and therefore cost savings.
A positive result is less conclusive and may need to be confirmed by subsequent invasive angiography.
The positive predictive value of cardiac CTA is approximately 82% and the negative predictive value is around 93%.
This means for every 100 patients who appear to have coronary artery disease after CT angiography, 18 of them actually won’t have it, and that for every 100 patients who have a negative CT angio test result 7 will actually have the disease as defined by the reference standard of invasive coronary angiography via cardiac catheterization.
Both coronary CT angiography and invasive angiography via cardiac catheterization yield similar diagnostic accuracy when both are being compared to a third reference standard such as intravascular ultrasound or fractional flow reserve.
Cardiac CT enables the visualization of the vessel wall, in a non-invasive manner, that can identify characteristics of coronary artery disease that are associated to the development of acute coronary syndrome.
For a patient with low to intermediate risk acute chest pain presented to the emergency department coronary CT angiography is a highly effective screening tool which shortens the length of stay in the emergency department and decreases rates of hospitalizations.
CT coronary angiography decreases time to diagnosis, and results in a more appropriate percutaneous coronary intervention, it decreases major adverse cardiac events including cardiac death of myocardial infarction.
Because the heart is effectively imaged more than once, cardiac CT angiography can result in a relatively high radiation exposure (around 12 millisievert), although newer protocols, have reduced this exposure to around 1 mSv.
By comparison, a chest X-ray carries a dose of approximately 0.02-0.2 mSv and natural background radiation exposure is around 2.3 mSv/year.
The potential risk of radiation must be weighed against the competing risk of not diagnosing a significant health problem in a particular individual, such as coronary artery disease.
Pregnancy is considered a relative contraindication.
When an iodine-containing contrast agent is used, severe contrast agent allergy, uncontrolled hyperthyroidism or renal function impairment are also relative contraindications.
Cardiac arrhythmias, coronary artery stents and tachycardia may result in a reduced image quality.
Improved resolution
Multi-slice CT (up to 320 slices), high resolution and high speed studies can be obtained, allowing excellent imaging of the coronary arteries.
Dual Source CT scanners, allow higher temporal resolution by acquiring a full CT slice in only half a rotation, thus reducing motion blurring at high heart rates and potentially allowing for shorter breath-hold time.
The speed advantages of 64-slice MSCT have rapidly established it as the minimum standard for newly installed CT scanners intended for cardiac scanning.
Introduction of a CT scanner with a 160 mm detector allows for imaging of the whole heart in a single beat without motion of the coronary arteries, regardless of patient heart rate.
The latest MSCT scanners acquire images only at 70-80% of the R-R interval (late diastole).
This prospective gating can reduce effective dose from 10 to 15 mSv to as little as 1.2 mSv in follow-up patients acquiring at 75% of the R-R interval.
Effective dose using MSCT coronary imaging can average less than the dose in conventional coronary angiography.
In the SCOT-HEART trial showed that the rate of death or non-fatal myocardial infarction was 40% lower when anatomical testing with CT angiography was the imaging method used than when stress testing was used.
With acute chest pain, CT angiography was compared with myocardial perfusion imaging, standard care, exercise treadmill testing, and high sensitivity troponin measurement: each study showed the superiority of CT angiography over the comparator with respect to cost, time to discharge, or both.
CT angiography is safe and results in lower cost ensure the length of hospital stay then those associated with the other approaches, most notably myocardial perfusion imaging.
CT angiography can access ischemic burden by estimating fractional flow reserve.
It is important a prognostic informer providing information on the anatomical and hemodynamic significance of stenosis.
Functional flow reserve-CT review and follow album affords better discrimination of ischemia than that are provided by other non-invasive tests including myocardial perfusion imaging and positron emission tomography.
Radiation doses are significantly lower with CT angiography then with myocardial perfusion imaging making it the preferred test for acute nonspecific chest pain.
CT angiography affords information related to stenosis including its location, calcification, length, complexity, and simultaneously the severity of underlying atherosclerosis.
Positive outcomes from multiple randomized trials favoring CT angiography calls for the function of imaging to be linked to the ability of CT angiography to identify nonobstructive coronary disease, leading to increased use it is it therapy search statins, aspirin, and angiotensin converting enzyme inhibitors as well as improved adherence to these therapies.
Among patients with stable chest pain and intermediate pretest probability of coronary artery disease, the risk of major adverse cardiovascular events is similar in a CT group and in an invasive coronary angiography group: the frequency of major procedure related complications is lower with an initial CT scan strategy (The DISCHARGE trial group).